[ad_1]
Background
Bacterial vaginosis is a prevalent microbiological condition of the vaginal flora in sexually active women. The typical vaginal flora has changed. Due to the decline in lactobacilli and the rise in other anaerobic microbes, it is a polymicrobial illness. Pregnancy-related bacterial vaginosis is linked to an increased risk of preterm birth, early membrane rupture, and chorioamnionitis owing to ascending infection. They have found amniotic fluid and placenta-derived bacteria in pregnant women who delivered prematurely. Cervicitis, salpingitis, endometritis, post-operative infections, and oophoritis are among the gynecologic consequences of bacterial vaginosis. Geographical, socioeconomic, and clinical characteristics of the population all affect the incidence of BV among pregnant women, and these differences are seen all over the world. Prevalence of BV among pregnant women varies from 9.3% to 17% in high-income nations.1,2 There have been reports of incidence rates in Africa as low as 6.4% in Burkina Faso and as high as 38% in Botswana.3,4 Most sub-Saharan nations have reported high prevalence rates; in Botswana, Zimbabwe, Kenya, and Ethiopia, those rates are 38%, 32.5%, 20.6%, and 19.4%, respectively.4–7
The diverse bacterial community that lives in the human vagina in the lower genital tract is known as the vaginal microbiome, and it plays a crucial role in the reproductive and newborn health of women. Dysbiosis, a term for imbalances in this microbiota, has been linked to several harmful conditions, including bacterial vaginosis (BV), increased susceptibility to pelvic inflammatory disease, and increased transmission of sexually transmitted pathogens like Chlamydia trachomatis, Neisseria gonorrhoeae, and HIV.8,9 Currently, Lactobacillus spp. the colonization of the vaginal microbiome in women of reproductive age is considered healthy. By adhering to mucus, creating a barrier that hinders pathogen colonization, and producing antimicrobial substances such as lactic acid, hydrogen peroxide, bacteriocins, and biosurfactants, lactobacilli are known to inhibit pathogen development.10 To maintain vaginal microbiome homeostasis, lactobacilli are considered to produce lactic acid.11,12
Bacterial vaginosis is the most prevalent gynecological disorder in women of reproductive age globally, which is characterized by a change from normal lactobacilli to an anaerobic overgrowth of many species, including Gardnerella vaginalis, Bacteroides spp., and Mobiluncus spp.13,14 The Nugent score,15 which is based on a scoring system that represents the relative number of bacterial cell morphotypes in Gram-stained vaginal smears, is the current gold standard approach for the diagnosis of BV. The Nugent score does not accurately identify and quantify bacteria at the species level while being rapid and affordable.
Microbiome dysbiosis and BV have been linked to various poor reproductive outcomes in pregnancy, with preterm delivery being the most frequent.16,17 Prematurity is a complicated multifactorial disease, which is highlighted by the fact that no one bacterial or collection of bacteria has yet been directly linked to this condition. Furthermore, there is still a lack of knowledge regarding the mechanisms underlying changes in the composition of the vaginal microbiota and the causes of microbiome imbalances in pregnant or non-pregnant women. This highlights the need for more effective methods to study the vaginal microbial community in health and “disease”.
Nugent, Krohn, and Hillier’s microbiological criteria are the gold standard for BV diagnosis.15 The Nugent score is based on a numerical scoring scale (0–10), with a score of 0–3 indicating health, a score of 4–6 denoting intermediate status, and a score of 7–10 denoting BV. Large Gram-positive rods (Lactobacillus), tiny Gram-negative and Gram variable rods (Gardnerella vaginalis/Bacteroides spp.), and curved Gram-negative rods (Mobiluncus) are the three types of bacterial cell morphotypes that are represented by the score in Gram-stained vaginal smears.15 The clinical criteria developed by Amsel et al in 1983 may also be used to determine if a woman has bacterial vaginosis. BV is defined by the presence of at least three of the following four criteria: Thin, grey or white discharge; unpleasant, “fishy” discharge after adding 10% potassium hydroxide; high vaginal pH (>4.5); and detection of vaginal epithelial cells extensively contaminated with bacteria (also known as “clue cells”) are some of the symptoms of vaginal infection.18
A few culture-independent studies investigated the vaginal microbiomes of healthy pregnant and non-pregnant women in light of the hormonal and physiological changes related to pregnancy. Compared to non-pregnant women, pregnant women’s microbiomes are generally less varied and rich.19,20 Pregnant women also have greater levels of Lactobacillus spp. and are more stable. The hypothesis that pregnancy has a transitory impact on the vaginal microbial community is supported by the fact that post-partum microbiomes become less Lactobacillus-dominating and richer and more diversified (ie, more comparable to the microbiomes of non-pregnant women) after delivery.20 When compared to non-pregnant women, pregnant women have greater glycogen deposition due to the higher amounts of estrogen that are present throughout pregnancy.21 As previously reported, the production of lactic acid by Lactobacillus from glycogen has a protective effect against low vaginal pH.11,22 Our study aimed to describe the characteristics and presenting manifestations of bacterial vaginosis in pregnant women and its association with dyspareunia and dysuria.
Methods
This study adapted an analytical questionnaire-based cross-sectional study design. The data were collected during the period from May 2023 to July 2023. The study included data from married pregnant Saudi women who have been diagnosed with bacterial vaginosis and agree to participate in study. The study excluded all women who are living abroad or are still single.
A self-administered questionnaire was used for data collection. The questionnaire comprised information regarding coexisting medical conditions, presenting symptoms, and outcome of treatment. The Statistical Package for Social Sciences (SPSS) version 26 was used for data management and analysis. We used Chi-square test for inferential analyses where a p-value equal to or less than 0.05 was considered significant.
The ethical approval was obtained from Scientific Research Ethical Committee at Najran University with reference No: 012141-027266DS prior to the study. We did not include names or other personal identifying data. Written informed consent was taken from patient prior to study. The research complies with the Declaration of Helsinki.
Results
The study included 456 women, whose age ranged from 19 to 46 years. The majority were 19 to 29 years old (61.9%) and had a university degree (73.3%). The prevalence of smoking was 2.2%, obesity was 22.9%, hypertension was 1.6%, and diabetes mellitus was 3.3% (Table 1).
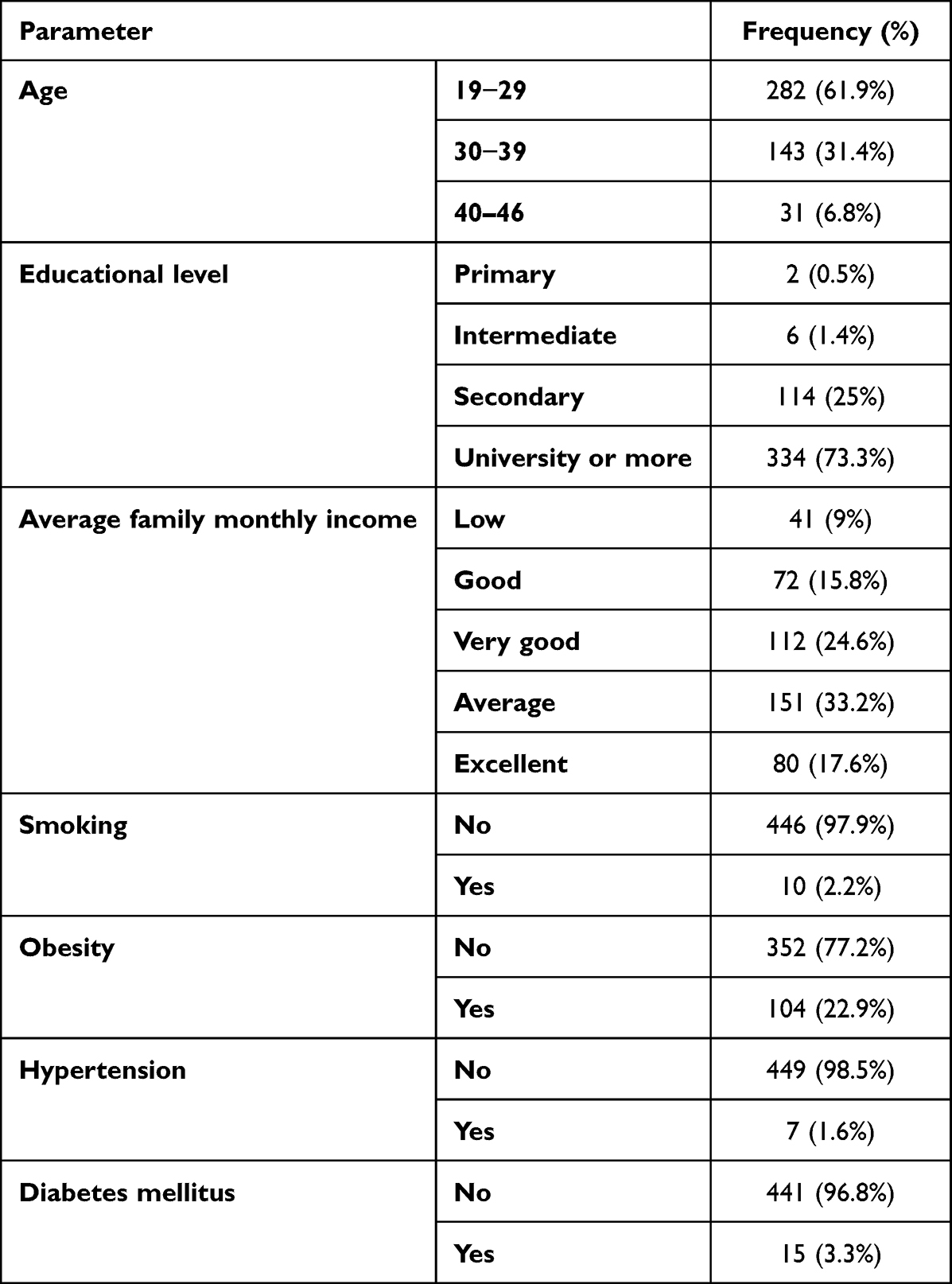 |
Table 1 Characters of Participating Women (n = 456) |
As shown in Table 2, vulval itching was reported by 59.7%, swelling by 7.7%, increased secretions by 81%, dyspareunia by 62.5%, and burning micturition by 44.6%. Yellowish secretions were reported by 31% of the participants, and bad odour was reported by 32.1%. The majority (92.8%) referred to medical advice and 97.9% were prescribed medications, where 82.5% improved on medications.
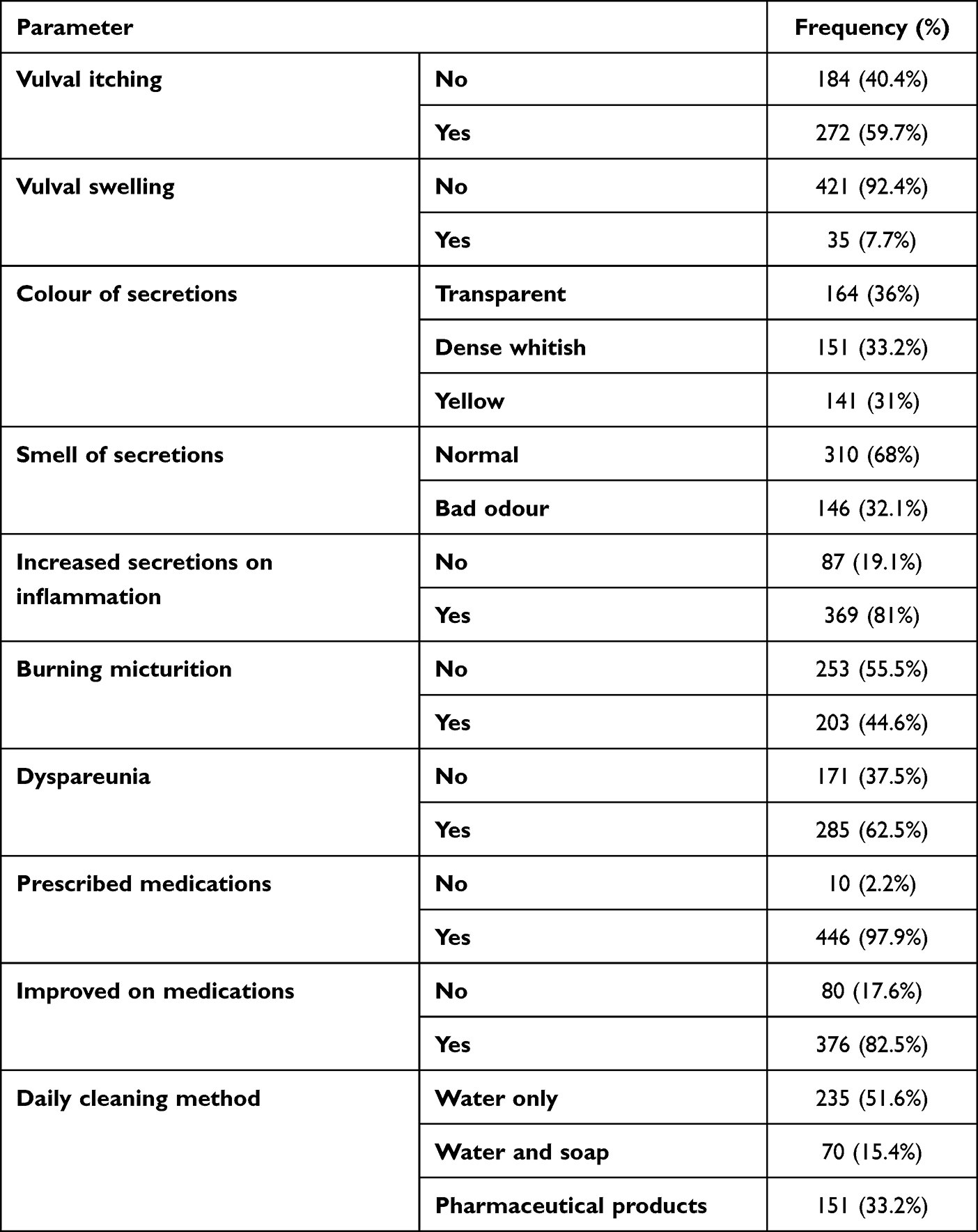 |
Table 2 Symptoms and Complaints of Bacterial Vaginosis Among Participants (n = 456) |
Table 3 shows the association between dyspareunia and burning micturition and other presenting symptoms. Dyspareunia was significantly more common in older (67.7%), and younger (66.7%) age groups (p = 0.020), women who are not obese (66.2%; p = 0.003), women with vulval swelling (94.3%; p = 0.000), women with vulval itching (66.2%; p = 0.049), women with dense whitish secretions (72.8%; p = 0.002), and women with less secretions (90.8%; p = 0.000).
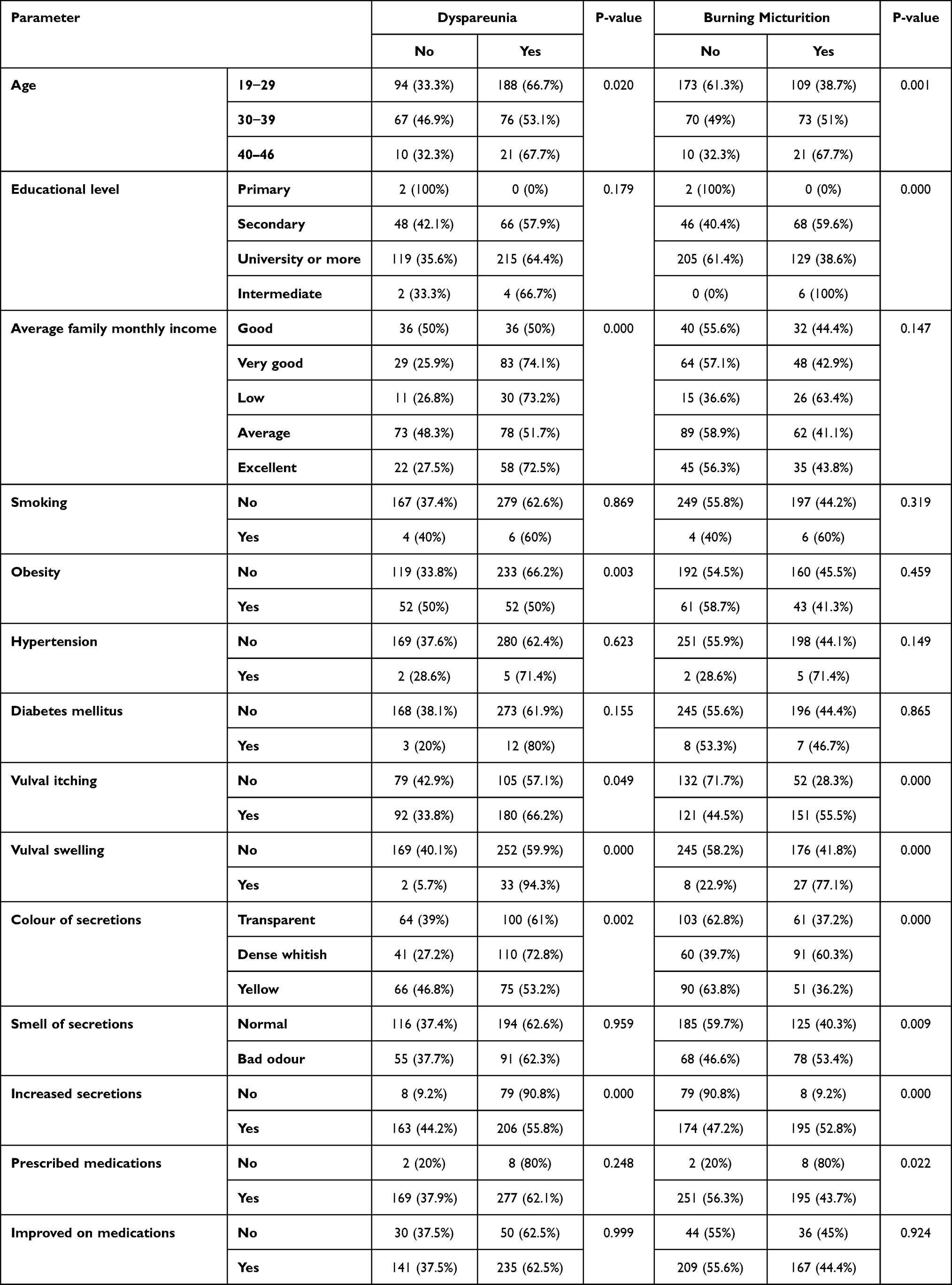 |
Table 3 Dyspareunia and Burning Micturition in Association with Characters and Symptoms of Bacterial Vaginosis (n = 456) |
Burning micturition was significantly more common among older women (p = 0.001), women with lower educational level (p = 0.000), women with vaginal itching and swelling (p = 0.000), those who have dense white secretions (p = 0.000) with bad odour (p = 0.009), women who were not prescribed medications (p = 0.022), and those with increased secretions (p = 0.000).
Discussion
Bacterial vaginosis is one of the most frequent vaginal tract infections during pregnancy, particularly so in the African population. The condition is characterised by elevated vaginal pH, milky, creamy discharge, and an amine- or fishy-smelling odour. It is characterised by a change in the vaginal flora, which goes from being dominated by the Lactobacillus species to being mixed.23
Due to variations in the geographic, socioeconomic, and clinical features of the study populations, it has been shown that the severity and determinants of BV vary from one location to another. Age, race, socioeconomic level, smoking, vaginal douching, sexual activity, many sexual partners, history of current or prior Sexually Transmitted Diseases (STIs), and infection with the Human Immunodeficiency Virus are some of the variables that have been linked to the cause of BV (HIV).6,23,24 Our study aimed to describe the characters and presenting manifestations of bacterial vaginosis in pregnant women.
Our study included 456 women and found that 59.7% of people felt vulval itching, 7.7% reported swelling, 81% reported increased secretions, 62.5% reported dyspareunia, and 44.6% reported burning micturition. Thirty-one percent of individuals reported yellowish discharges, while 32.1% reported foul odour. The majority (92.8%) made use of medical advice, and 97.9% were given prescriptions for drugs, where 82.5% were better than the medication.
Older women (p = 0.001), those with lower educational levels (p = 0.000), those with vaginal itching and swelling (p = 0.000), those with dense white secretions (p = 0.000), those with bad odours (p = 0.009), those who were not prescribed medications (p = 0.022), and those with increased secretions (p = 0.000) all had significantly higher rates of burning urination.
Bacterial vaginosis is associated with poor maternal and perinatal outcomes, including chorioamnionitis, postpartum endometritis, spontaneous abortion, preterm labour (PTL), premature membrane rupture (PROM), low birth weight infants, neonatal sepsis, and mortality. Early in pregnancy or even before to conception, intrauterine infections may happen and go unnoticed for months until PTL or PROM. One of the most difficult obstetric problems is preterm labour and delivery.25,26
Our study reported a 44.5% prevalence of dysuria among participants with bacterial vaginosis. It was observed in 1989 that women who use diaphragms had a connection between bacterial vaginosis and urinary tract infections.27 A paper from 2000 claimed that women with bacterial vaginosis (BV) were more likely than others to get urinary tract infections.28 The same researchers revealed the connection between bacterial vaginosis and urinary tract infections in pregnant women in 2002.
The prevalence of dyspareunia was significantly higher in the older (67.7%) and younger (66.7%) age groups (p = 0.020), in non-obese women (p = 0.003), in women with vulval swelling (p = 0.000), in women with vulval itching (p = 0.049), in women with dense whitish secretions (p = 0.002), and in women with fewer secretions (p = 0.000). In a cross-sectional study,28 we looked at 503 pregnant women who were coming in for their first prenatal visit from the perspectives of urinary tract infections and BV. They found that 13.6% of the 140 women with BV also had urinary tract infections (UTI), but only 6.6% of the 363 women without BV did. According to their findings, BV during pregnancy increases the risk of UTI.28 In a case–control study,29 we looked at 67 UTI patients and compared them to 67 healthy people. In the control group and research group, BV was noted in 40.3% and 62.7% of cases, respectively.29
The relationship between BV and UTI (and vice versa) likely starts with a rise in vaginal pH due to a decrease in the vaginal lactobacilli that produces lactate and hydrogen peroxide. A flora that is mostly anaerobic may take the place of the usual vaginal flora.28 Frequent sex sessions, which were connected to both of these diseases, might be a factor in these phenomena.30 Although the exact causes of gram-negative bacilli colonisation around urethra are unknown, it appears that urethral massage during sexual activity plays a facilitative role. Additionally, it appears that the urethra’s proximity to the anus, shortness in females, location under the labia, and the warm and moist environment of the perineum play significant roles. Women with bacterial vaginosis may need to undergo testing for urinary tract infections (vice versa). In light of the potential reduction in the risk of related sequelae, checking for urinary tract infections in women with bacterial vaginosis is cost-effective. Given the potential perinatal issues these infections might cause, clinical care in expectant women may be more difficult.31 More research is required to determine the precise order of occurrences.
Conclusion
According to the results of our study, dyspareunia and dysuria were significantly linked with the majority of the presenting symptoms. The study also shows that with the prescribed treatment, nearly all participants made a full recovery. Since bacterial vaginosis may be treated and is a preventable cause of difficult pregnancies, we advise healthcare systems to carefully diagnose and treat the condition.
Disclosure
The author has no conflict of interest to declare.
References
1. Larsson PG, Fåhraeus L, Carlsson B, Jakobsson T, Forsum U. Predisposing factors for bacterial vaginosis, treatment efficacy and pregnancy outcome among term deliveries; results from a preterm delivery study. BMC Womens Health. 2007;7:20. doi:10.1186/1472-6874-7-20
2. Vogel I, Thorsen P, Jeune B, et al. Acquisition and elimination of bacterial vaginosis during pregnancy: a Danish population-based study. Infect Dis Obstet Gynecol. 2006;2006:94646. doi:10.1155/IDOG/2006/94646
3. Kirakoya-Samadoulougou F, Nagot N, Defer MC, Yaro S, Meda N, Robert A. Bacterial vaginosis among pregnant women in Burkina Faso. Sex Transm Dis. 2008;35(12):985–989. doi:10.1097/OLQ.0b013e3181844f22
4. Romoren M, Velauthapillai M, Rahman M, Sundby J, Klouman E, Hjortdahl P. Trichomoniasis and bacterial vaginosis in pregnancy: inadequately managed with the syndromic approach. Bull World Health Organ. 2007;85(4):297–304. doi:10.2471/blt.06.031922
5. Kurewa NE, Mapingure MP, Munjoma MW, et al. The burden and risk factors of sexually transmitted infections and reproductive tract infections among pregnant women in Zimbabwe. BMC Infect Dis. 2010;10(1):127. doi:10.1186/1471-2334-10-127
6. Mengistie Z, Woldeamanuel Y, Asrat D, et al. Prevalence of bacterial vaginosis among pregnant women attending antenatal care in Tikur Anbessa University Hospital, Addis Ababa, Ethiopia. BMC Res Notes. 2014;7(1):822. doi:10.1186/1756-0500-7-822
7. Thomas T, Choudhri S, Kariuki C, Moses S. Identifying cervical infection among pregnant women in Nairobi, Kenya: limitations of risk assessment and symptom-based approaches. Genitourin Med. 1996;72(5):334–338. doi:10.1136/sti.72.5.334
8. Borgdorff H, Gautam R, Armstrong SD, et al. Cervicovaginal microbiome dysbiosis is associated with proteome changes related to alterations of the cervicovaginal mucosal barrier. Mucosal Immunol. 2016;9(3):621–633. doi:10.1038/mi.2015.86
9. Wiesenfeld HC, Hillier SL, Krohn MA, Landers DV, Sweet RL. Bacterial vaginosis is a strong predictor of Neisseria gonorrhoeae and Chlamydia trachomatis infection. Clin Infect Dis. 2003;36(5):663–668. doi:10.1086/367658
10. Boris S, Barbés C. Role played by lactobacilli in controlling the population of vaginal pathogens. Microbes Infect. 2000;2(5):543–546. doi:10.1016/s1286-4579(00)00313-0
11. O’Hanlon DE, Moench TR, Cone RA, Landay A. Vaginal pH and microbicidal lactic acid when lactobacilli dominate the microbiota. PLoS One. 2013;8(11):e80074. doi:10.1371/journal.pone.0080074
12. Boskey ER, Telsch KM, Whaley KJ, Moench TR, Cone RA, McGhee JR. Acid production by vaginal flora in vitro is consistent with the rate and extent of vaginal acidification. Infect Immun. 1999;67(10):5170–5175. doi:10.1128/IAI.67.10.5170-5175.1999
13. Sobel JD. Bacterial vaginosis. Annu Rev Med. 2000;51(1):349–356. doi:10.1146/annurev.med.51.1.349
14. Hillier SL. Diagnostic microbiology of bacterial vaginosis. Am J Obstet Gynecol. 1993;169(2 Pt 2):455–459. doi:10.1016/0002-9378(93)90340-o
15. Nugent RP, Krohn MA, Hillier SL. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbiol. 1991;29(2):297–301. doi:10.1128/jcm.29.2.297-301.1991
16. Leitich H, Bodner-Adler B, Brunbauer M, Kaider A, Egarter C, Husslein P. Bacterial vaginosis as a risk factor for preterm delivery: a meta-analysis. Am J Obstet Gynecol. 2003;189(1):139–147. doi:10.1067/mob.2003.339
17. Meis PJ, Goldenberg RL, Mercer B, et al. The preterm prediction study: significance of vaginal infections. National Institute of child health and human development maternal-fetal medicine units network. Am J Obstet Gynecol. 1995;173(4):1231–1235. doi:10.1016/0002-9378(95)91360-2
18. Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am J Med. 1983;74(1):14–22. doi:10.1016/0002-9343(83)91112-9
19. Aagaard K, Riehle K, Ma J, et al. A metagenomic approach to characterization of the vaginal microbiome signature in pregnancy. PLoS One. 2012;7(6):e36466. doi:10.1371/journal.pone.0036466
20. MacIntyre DA, Chandiramani M, Lee YS, et al. The vaginal microbiome during pregnancy and the postpartum period in a European population. Sci Rep. 2015;5(1):
21. Cruickshank R, Sharman A. The biology of the vagina in the human subject. II the bacterial flora and secretion of the vagina at various age-periods and their relations to glycogen in the vaginal epitehlial. BJOG an Int J Obstet Gynaecol. 1934;41(2):190–207. doi:10.1111/j.1471-0528.1934.tb08758.x
22. Mirmonsef P, Hotton AL, Gilbert D, et al. Free glycogen in vaginal fluids is associated with Lactobacillus colonization and low vaginal pH. PLoS One. 2014;9(7):e102467. doi:10.1371/journal.pone.0102467
23. Kenyon C, Colebunders R, Crucitti T. The global epidemiology of bacterial vaginosis: a systematic review. Am J Obstet Gynecol. 2013;209(6):505–523. doi:10.1016/j.ajog.2013.05.006
24. Shayo PA, Kihunrwa A, Massinde AN, et al. Prevalence of bacterial vaginosis and associated factors among pregnant women attending at Bugando Medical Centre, Mwanza, Tanzania. Tanzan J Health Res. 2012;14(3):175–182. doi:10.4314/thrb.v14i3.3
25. Kurki T, Sivonen A, Renkonen OV, Savia E, Ylikorkala O. Bacterial vaginosis in early pregnancy and pregnancy outcome. Obstet Gynecol. 1992;80(2):173–177.
26. Eschenbach DA, Gravett MG, Chen KC, Hoyme UB, Holmes KK. Bacterial vaginosis during pregnancy. An association with prematurity and postpartum complications. Scand J Urol Nephrol Suppl. 1984;86:213–222.
27. Hooton TM, Fihn SD, Johnson C, Roberts PL, Stamm WE. Association between bacterial vaginosis and acute cystitis in women using diaphragms. Arch Intern Med. 1989;149(9):1932–1936. doi:10.1001/archinte.1989.00390090014003
28. Hillebrand L, Harmanli OH, Whiteman V, Khandelwal M. Urinary tract infections in pregnant women with bacterial vaginosis. Am J Obstet Gynecol. 2002;186(5):916–917. doi:10.1067/mob.2002.123987
29. Sharami SH, Afrakhteh M, Shakiba M. Urinary tract infections in pregnant women with bacterial vaginosis. J Obstet Gynaecol. 2007;27(3):252–254. doi:10.1080/01443610701194846
30. Harmanli OH, Cheng GY, Nyirjesy P, Chatwani A, Gaughan JP. Urinary tract infections in women with bacterial vaginosis. Obstet Gynecol. 2000;95(5):710–712. doi:10.1016/s0029-7844(99)00632-8
31. Trabert B, Misra DP. Risk factors for bacterial vaginosis during pregnancy among African American women. Am J Obstet Gynecol. 2007;197(5):477.e1–477.e4778. doi:10.1016/j.ajog.2007.03.085
[ad_2]
Source link