New targets, guidance reframe treatment of hypertensive disorders of pregnancy

[ad_1]
March 18, 2022
10 min read

Source/Disclosures
Published by:
Source:
Healio Interviews
Disclosures:
Garovic, Langen, Minissian and Sharma report no relevant financial disclosures. Minhas reports receiving a research grant from AMEC.
Hypertensive disorders of pregnancy are the second leading cause of maternal death behind maternal hemorrhage and are a significant cause of short- and long-term maternal and offspring morbidity worldwide.
Prior research indicates hypertension develops faster among women who experienced hypertensive disorders of pregnancy, up to 10 years earlier, compared with women with normotensive pregnancies.

Garima V. Sharma, MD, FACC, FACP, from Johns Hopkins University School of Medicine, discusses the risks of hypertensive disorders of pregnancy. Source: Toshal Roy. Printed with permission.
“In the setting of pregnancy, certain hypertensive disorders, in particular preeclampsia and eclampsia, are linked with adverse outcomes for mom and baby,” Garima V. Sharma, MD, FACC, FACP, assistant professor of medicine and director of the cardio-obstetrics program at Johns Hopkins University School of Medicine and a Cardiology Today Editorial Board Member, said in an interview. “That includes HF during pregnancy with pulmonary edema, seizures, strokes for the mother, babies born small for gestational age, premature birth and even stillbirth in very severe cases. It is important to recognize and treat to prevent those complications during pregnancy.”
In a scientific statement published in December in Hypertension, the American Heart Association stated high BP should be treated during pregnancy and treatment should be individualized to each patient, considering risk factors such as maternal age, race and comorbid conditions. Moreover, reclassifying hypertensive disorders of pregnancy with the lower American College of Cardiology/AHA diagnostic threshold of 130/80 mm Hg or more may better identify women at risk and prevent adverse hypertensive end-organ complications, according to the new guidance. That threshold for the general population is lower than what is currently posited by the American College of Obstetricians and Gynecologists (ACOG) and other societies — 140/90 mm Hg.

“There was a need for this statement because emerging data support the benefits and safety of BP treatment during pregnancy,” Vesna D. Garovic, MD, PhD, chair of the division of nephrology and hypertension with a joint appointment in the department of obstetrics and gynecology at Mayo Clinic and chair of the AHA statement writing committee, told Cardiology Today. “Despite most guidelines worldwide defining hypertension during pregnancy as 140/90 mm Hg or higher, there are significant discrepancies among the societies when it comes to proposing BP cutoffs, both for the initiation of therapy and the goals of therapy.”

Experts said they hope that the new guidance can reframe the debate around BP treatment timing and goals during pregnancy. Particularly for at-risk women, pregnancy offers an opportunity for clinicians to “get ahead” of adverse outcomes related to hypertensive disorders, according to Cardiology Today Editorial Board Member Margo B. Minissian, PhD, ACNP, NEA-BC, AACC, FAHA, FNLA, assistant professor of cardiology and director of the women’s heart health program at the Barbra Streisand Women’s Heart Center in the Smidt Heart Institute and executive director of the Geri and Richard Brawerman Nursing Institute at Cedars-Sinai.
“From a woman’s perspective, evaluating her birth course is a window into her cardiovascular future,” Minissian said. “About 86% of women have children. Pregnancy offers a perfect opportunity for us to evaluate women much earlier than we have been and instill cardiovascular prevention strategies early, instead of waiting until midlife when women may have already developed precursors of disease.”
Treatment timing controversies
Diagnostic BP treatment thresholds for the general population have evolved. In 2017, the ACC/AHA hypertension clinical practice guidelines lowered the threshold for the diagnosis of stage 1 hypertension to 130/80 mm Hg from 140/90 mm Hg. The decision was based on observational studies and clinical trials demonstrating reduced CV events with treatment to lower levels.
Such a change has been considered controversial for pregnant women. Most guidelines agree hypertension in pregnancy is defined as BP of 140/90 mm Hg or more; however, there is inconsistency regarding the threshold for initiation of antihypertensive treatment due to a lack of certainty of its benefits for this population.
“There is controversy about when to initiate treatment,” Elizabeth Suzanne Langen, MD, clinical associate professor of obstetrics and gynecology and co-director of the cardio-obstetrics program at the University of Michigan, told Cardiology Today. “I work very closely with cardiologists in our cardio-obstetrics program. We have ongoing conversations about what our BP target is and how we should treat. We consider fetal status and mom’s history, but I think the ‘right’ number is not known. I appreciate that the AHA is asking us to question BP targets which have been etched in stone for a long time.”

The new AHA statement is timely. The incidence of hypertensive disorders of pregnancy continues to increase, in part due to more women becoming pregnant for the first time at an older age, along with an increased prevalence of obesity and other cardiometabolic risk factors. Data show pregnancy-related stroke hospitalizations increased by 60% from 1994 to 2011, Garovic said. Hypertensive disorders of pregnancy-associated stroke rates increased twofold compared with stroke not related to such disorders.
“The demographics are changing; now, we see more women of advanced age getting pregnant,” Garovic said. “This is not a typical 20-year-old who developed preeclampsia and is otherwise healthy. Now we are often talking about a woman who is age 40 years or older, with history of hypertension, heart disease, metabolic syndrome, diabetes. The risks for hypertension for that woman are quite different than the risk for hypertension in a young woman who is otherwise healthy and without any coexisting risks.”
‘Treat them or give them tools’
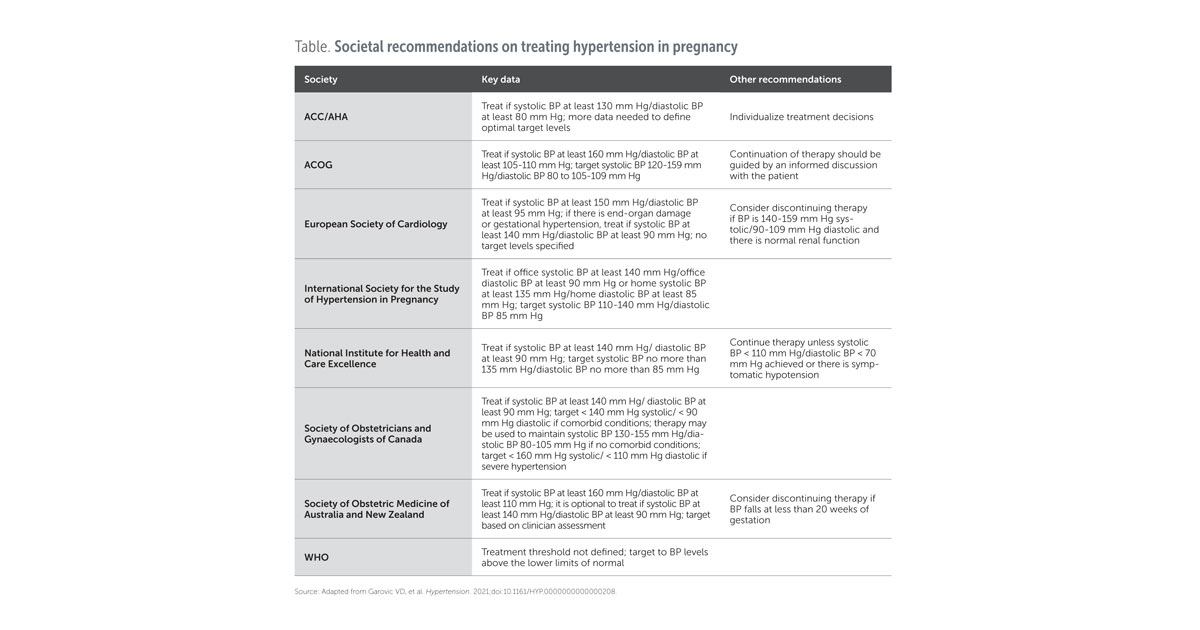
The ACOG recommends antihypertensive therapy for women with preeclampsia or chronic hypertension with a sustained BP of 160/110 mm Hg, with a treatment goal of 120-160/80-110 mm Hg.
Internationally, most hypertension societies endorse a more aggressive approach for antihypertensive treatment, recommending therapy when BP is at least 140/90 mm Hg. The International Society for the Study of Hypertension in Pregnancy, Hypertension Canada Guidelines, National Institute for Health and Care Excellence and WHO recommend therapeutic targets like the ACC/AHA target of 130/80 mm Hg (Table).
“I tend to keep a close eye on BP and treat each patient on a case-by-case basis and do it in consultation with our MFM colleagues,” Sharma said. “If someone has elevated BP in the 150s over 100s, that can very easily become 160/110 mm Hg and turn into renal failure and heart failure. This is where self-monitoring of BP with ambulatory or home BP cuffs is very helpful.”
Initial antihypertensive therapy is widely established to be monotherapy with an accepted first-line drug: labetalol or methyldopa. Some guidelines also support the use of nifedipine as an initial therapy. According to the AHA statement, reviews of trial data show there is no clear evidence that one drug is preferable to another.
The beta-blocker atenolol is not recommended; data from a meta-analysis suggested it was associated with fetal growth restriction, especially when given for a longer duration.
“If a woman has no other comorbidities, then we individualize treatment based on patient preference or convenience of use,” Anum Minhas, MD, MHS, chief cardiology fellow at Johns Hopkins Heart and Vascular Institute, told Cardiology Today. “Is the patient willing to take a twice-daily medication? If not, then those are excluded from the options. Has that patient experienced adverse effects with any of the treatments you are recommending? For example, nifedipine is a common antihypertensive in pregnancy, but it is more likely to cause swelling in the legs.”

The ACOG and the International Society for the Study of Hypertension in Pregnancy also recommend the use of self-measured BP in women with chronic or gestational hypertension, particularly when uncontrolled, though researchers caution additional information on appropriate methodology and validation of BP devices is needed.
“We can treat them or give them the tools,” Sharma said. “You don’t want to alarm the mother, but if they have BPs in the 130/90 mm Hg range, that is high for that mother during pregnancy based on her previous BP. She needs to monitor it. Provide her with a BP monitor. Tell her to start noting her BP, maintain a log and call if she is noticing BP trends go up. There are medicines that can be used safely in pregnancy. We have good data on labetalol and nifedipine and have found them to be effective and safe. These are drugs that have been around for many years.”
Addressing social determinants
Hypertensive disorders of pregnancy disproportionally affect Black, American Indian and Alaska Native women, according to CDC data, predominantly because of the overall higher prevalence of CVD risk factors. However, evidence also suggests biological factors, such as specific genetic variants, may increase risk for preeclampsia for Black women. Preeclampsia-related severe morbidity and mortality are higher for Black women, whereas for Hispanic women, pregnancy outcomes tend to be better than those of Black or white women of similar risk.
A recent systematic review published in Obstetrics & Gynecology showed Black, American Indian and Alaska Native women tend to have poorer social determinants of health, loosely defined as conditions in the environments where people are born, live, learn and work.
Data demonstrating the stark differences in maternal outcomes for underserved and underrepresented women, particularly those with hypertensive disorders during pregnancy, are causing some providers to rethink how they provide care.
“I have done prenatal visits with folks who are on their break at work because they cannot get time off work, but they can get 15 minutes of a break,” Langen said.
Minissian said she and her team are enrolling postpartum women into a research study to closely follow patients who do not qualify for other programs.
“For women receiving Medicaid, they get one postpartum visit. That’s it,” Minissian said. “They do not have admission into my postpartum heart health program. The only way I can reach them is to enroll them into a research study. We created a registry and a biorepository, so at least we can be in contact with them annually.”
“When we talk about maternal health and reducing maternal mortality, which is unfortunately rising in the United States, it goes well beyond the hospital system,” Minhas said. “It goes into the legal implications of providing Medicaid coverage beyond 60 days postpartum. It goes into the social changes, addressing food insecurity and access to child care. It even goes into pediatrician visits for those moms.”
Postpartum concerns, care
In a study published in November in the Journal of Women’s Health, only 13.7% of women diagnosed with a hypertensive disorder of pregnancy attended a BP screening within 7 to 10 days of delivery, despite recommendations to do so. BP typically declines immediately after delivery and then rises, peaking between 3 and 6 days postpartum — after most women have been discharged from the hospital.
“Especially during the postpartum period, women often will not go to obstetrical providers; they may show up to the ED or urgent care,” Langen said. “It is important providers in those settings know that for a young, postpartum person, having a BP that is high is a big deal. You cannot write that off as just stress or anxiety because the mother is not sleeping with a newborn.”
International guidelines emphasize the need for appropriate postpartum screening and control of CV risk factors for women with a history of preeclampsia. However, the lack of studies demonstrating efficacy and effectiveness of counseling and interventions in formerly preeclamptic women impedes the development of evidence-based guidelines, according to Garovic.
Sharma said it is crucial for providers to partner with community or institution resources, leveraging faith-based organizations, patient navigators or telehealth tools to follow up with women postpartum — particularly underserved women from marginalized communities.
“These women are at high risk for having hypertension postpartum, but what if they cannot come to your office?” Sharma said. “We need to educate our patients, telling them, ‘If you can’t come [to a follow-up appointment], our nurse is going to call you and we are going to give you the tools.’ It could be a telephone visit. Innovative health care delivery models that incorporate telemedicine and mobile app-based report BP monitoring can reduce some of the disparities and help.”
Minissian said good communication and listening to new mothers’ fears and concerns are another integral part of postpartum care.
“Some of these young women go home, leaving behind a baby in the neonatal ICU, and they are prescribed pills that they heard their grandpa took before he died, and they thought they were absolutely fine and were expecting to have this perfect vaginal delivery plan,” Minissian said. “It doesn’t always go the way that they hope. There is a lot to unpack around that. Many women have feelings of guilt, depression, anxiety and posttraumatic stress.”
‘Optimize what we know’
Researchers continue to evaluate whether a BP treatment strategy during pregnancy to achieve targets for nonpregnant, reproductive-age adults is effective and safe compared with ACOG-recommended standards. The ongoing CHAP study, initiated in 2015, includes more than 2,400 participants randomly assigned labetalol or nifedipine with a treatment goal of less than 140/90 mm Hg or no treatment unless BP is severe. Results are expected later this year.
“We are all nervously awaiting results of that trial,” Garovic said. “It is critically important to determine which BP levels during and post-pregnancy, both for starting therapy and treatment goals, are beneficial for the mother and safe for the fetus. It is still an open question.”
Other open questions remain.
“We do not really understand what underlying mechanistic issue causes preeclampsia,” Sharma said. “We know there are women at high risk for developing preeclampsia, but future studies must focus on the epigenetic, transcriptomic aspects of understanding the phenotypes of preeclampsia. We need to take this opportunity to educate women on the risks for long-term premature CVD, regardless of severity of hypertensive disorders in pregnancy.”
As research continues, there are steps clinicians can take to better identify women at higher risk for hypertensive disorders of pregnancy during prenatal visits, Minissian said.
“We need to optimize what we do know that helps us inform young women to take the healthy pathway moving forward,” Minissian said. “We can completely alter someone’s health trajectory by teaching them about the implications of smoking, the importance of exercising and maintaining a healthy weight or talking with your doctor if you see a BP greater than 130/80 mm Hg. Oftentimes these young women have elevated BPs that are blamed on being a young mother who is back to work and under stress. Then, they are not evaluated, screened and treated. Hypertension in this population can occur up to 10 years earlier than among women who do not have hypertension during pregnancy. The key is to keep your eyes open.”
- References:
- Campbell A, et al. J Womens Health (Larchmt). 2021;doi:10.1089/jwh.2021.0161.
- Chronic Hypertension and Pregnancy (CHAP) Project. Available at: clinicaltrials.gov/ct2/show/NCT02299414. Accessed Feb. 14, 2022.
- Garovic VD, et al. Hypertension. 2021;doi:10.1161/HYP.0000000000000208.
- High blood pressure treatment in pregnancy is safe, prevents maternal heart risks. www.newsroom.heart.org/news/high-blood-pressure-treatment-in-pregnancy-is-safe-prevents-maternal-heart-risks. Published Dec. 15, 2021. Accessed Feb. 14, 2022.
- Mehta LS, et al. Circulation. 2021;doi:10.1161/CIR.00000000000001000.
- For more information:
- Vesna D. Garovic, MD, PhD, can be reached at garovic.vesna@mayo.edu.
- Elizabeth Suzanne Langen, MD, can be reached at elangen@med.umich.edu; Twitter: @langenelizabeth.
- Anum Minhas, MD, MHS, can be reached at aminhas2@jhmi.edu; Twitter: @dranumminhas.
- Margo B. Minissian, PhD, ACNP, NEA-BC, AACC, FAHA, FNLA, can be reached at margo.minissian@cshs.org; Twitter: @minissianm.
- Garima V. Sharma, MD, FACC, FACP, can be reached at gsharma8@jhmi.edu; Twitter: @garimavsharmamd.
[ad_2]
Source link