[ad_1]
Larry R Jackson II,1 Daniel J Friedman,1 Diane M Francis,2 Sonia Maccioni,2 Vincent C Thomas,3 Paul Coplan,4 Rahul Khanna,4 Charlene Wong,4 Neloufar Rahai,4 Jonathan P Piccini1
1Division of Cardiology, Duke University Medical Center & Duke Clinical Research Institute, Durham, NC, USA; 2Health Economics and Market Access, Johnson & Johnson Medical Devices, Irvine, CA, USA; 3Medical Safety, Biosense Webster, Irvine, CA, USA; 4Medical Device Epidemiology and Real-World Data Sciences, Johnson & Johnson, New Brunswick, NJ, USA
Correspondence: Larry R Jackson II, Duke Clinical Research Institute, 300 W. Morgan Street, Durham, NC, 27701, USA, Tel +1 919-684-9940, Email [email protected]
Background: Atrial fibrillation (AF) is associated with considerable morbidity and mortality. Timely management and treatment is critical in alleviating AF disease burden. Variation in treatment by race and ethnic and sex could lead to inequities in health outcomes.
Objective: To identify racial and ethnic and sex differences in rhythm treatment for patients with incident AF.
Methods: Using 2010– 2019 Optum Clinformatics database, an administrative claims data for commercially insured patients in the United States (US), incident AF patients ≥ 20 years old who were continuously enrolled 12-months pre- and post-index diagnosis were identified. Rhythm control treatment (ablation, antiarrhythmic drugs [AAD], and cardioversion) for AF were compared by patient race and ethnicity (Asian, Hispanic, Black vs White) and sex (female vs male). Multivariable regression analysis was used to examine the relationship of race and ethnicity and sex with rhythm control AF treatment.
Results: A total of 77,932 patients were identified with incident AF. Black and Hispanic female patients had the highest CHA2DS2VASc scores (4.3 ± 1.8) and Elixhauser scores (4.1 ± 2.8 and 4.0 ± 6.7), respectively. Black males were less likely to receive AAD treatment (adjusted odds ratio [aOR] 0.87; 95% confidence interval [CI], 0.79– 0.96) or ablation (aOR, 0.72; 95% CI, 0.58– 0.90). Compared to White males, all groups had lower likelihood of receiving cardioversion with Asian females having the lowest [aOR, 0.48; 95% CI, (0.37– 0.63)].
Conclusion: Black patients were less likely to receive pharmacologic and procedural rhythm control therapies. Further research is needed to understand the drivers of undertreatment among racial and ethnic groups and females with AF.
Introduction
Atrial fibrillation (AF) is the most common abnormal heart rhythm disorder in the United States (US).1 Approximately 6 million individuals have AF in the US, with the prevalence of AF expected to increase to 16 million by 2050.2–4 Antiarrhythmic drug (AAD) therapy and catheter ablation are rhythm control strategies implemented to prevent recurrent AF and maintain sinus rhythm. Results from a multi-center trial, the Early Treatment of Atrial Fibrillation for Stroke Prevention Trial (EAST-AFNET 4), demonstrated benefits of early rhythm control including improved cardiovascular outcomes in AF patients.5 Guidelines from the 2017 American College of Cardiology, the American Heart Association, and the Heart Rhythm Society recommend catheter ablation as the first-line therapy for patients with recurrent symptomatic paroxysmal and persistent AF prior to trial of Class I or III AAD.6
Prior studies have observed racial and ethnic and sex differences in the treatment of AF. For example, White patients with AF are more likely to undergo catheter ablation than Black, Hispanic, Asian, or other racial and ethnic groups.7–15 Differences in treatment among males and females have also been noted, with female patients less likely to undergo catheter ablation for rhythm control of AF.6–14 A recent study by Eberly et al examined the relationship of race and ethnicity and socioeconomic status with use of a rhythm control strategy among patients with AF and demonstrated a significantly (P<0.001) lower likelihood of use of a rhythm control strategy in Black patients (versus White patients) and lower utilization of catheter ablation in patients of Latinx ethnicity (versus White patients) (P=0.002).15
With few exceptions, most of the extant literature on racial, ethnic, and sex differences in AF management is dated and does not provide current assessments of whether these differences have resolved, persist, or have been accentuated over time. As the treatment options have expanded, including technological advances in catheter ablation techniques which have led to improved effectiveness, there is an urgent need to re-evaluate racial and ethnic and sex differences in AF treatment using contemporary data. Though Eberly et al examined variation in AF treatment using a more contemporary data (2015–2019 period),16 they examined the topic from an individual prism of race and ethnicity or sex, but not as a collective function (ie, intersection of race and ethnicity and sex). As such, the objective of this study was to examine the intersection of racial and ethnic (White, Black, Asian, Hispanic, others) and sex (male, female) variation in the proportion of patients with incident (ie, newly diagnosed) AF receiving rhythm control, including AAD therapy, catheter ablation and cardioversion.
Methods
Data Source and Study Sample
We used the deidentified Optum Clinformatics Data Mart, Extended – Socioeconomic Status (Optum) from January 1, 2010 to December 31, 2019, to investigate the study objectives; years of data used included baseline and follow-up periods. The Optum database comprises health insurance claims data for a combination of US private insurance and Medicare Advantage beneficiaries from geographically diverse regions across the country. This database contains deidentified data derived from health plan members’ enrollment data and facility, physician, and pharmacy claims for approximately 13 million covered lives annually. In the Optum database, about 4% of the observations were missing information on race, and 0.02% were missing information on sex.
Patients who met all of the following criteria were included in the study: 1) had at least two medical service visits (within 3 months) between January 1, 2011 and December 31, 2018, with a primary diagnosis of AF (The International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9] code 427.31 and 10 Revision [ICD-10] codes I48.0, I48.1, I48.2, I48.91); one or more codes were required for the diagnosis of AF with the first such occurrence classified as index AF diagnosis; 2) had continuous enrollment 12-months pre- and post-index diagnosis; and 3) were ≥20 years of age at the time of index diagnosis. Patients who met any of the following were excluded from the study: 1) had AF diagnosis (primary or secondary) in the 12-month pre-index diagnosis period; 2) filled an AAD prescription in the 12-month pre-index diagnosis period; 3) had a history of congenital heart disease; and 4) had missing data for race or sex.
Study Variables
The primary independent variables of interest included patient race and ethnicity and sex. Covariates, selected based on prior AF research and theoretical plausibility, included age, insurance type, education, and clinical characteristics, including obstructive sleep apnea, Elixhauser comorbidity score, CHA2DS2-VASc score, and provider region as described in Table 1. Elixhauser comorbidity score was determined based on ICD-9 and ICD-10 diagnostic codes for 31 comorbid categories.17 Stroke risk was assessed using CHA2DS2-VASc scores, categorized as follows: score of 0, score of 1–3, and score of ≥4.18
 |
Table 1 Baseline Demographics of Patients with Incident Atrial Fibrillation |
The following healthcare and treatment utilization outcomes were assessed in the 1 year following the diagnosis of incident (newly diagnosed) AF: 1) use of one or more of the following AADs: Amiodarone, Dofetilide, Flecainide, Propafenone, Ibutilide, Sotalol, Dronedarone, Quinidine, and Disopyramide according to the National Drug Code directory; 2) receipt of catheter ablation treatment for AF, determined based on ICD-9, ICD-10, and Current Procedural Terminology (CPT) code (per previous studies,19,20 one or more codes were required for identification of treatment with catheter ablation, as shown in eTable 1); 3) receipt of cardioversion that was determined based on ICD-9 and ICD-10 (one or more codes were required for identification of treatment with cardioversion, as shown in eTable 1).
Data Analyses
Baseline characteristics are summarized using means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Chi-square tests were used to compare the proportion of patients, by race and ethnicity and sex, receiving AADs, ablation procedure, or cardioversion for AF treatment.
Multivariable logistic regression was used to determine associations between race and ethnicity and sex and rhythm treatment (AAD use, AF ablation, and cardioversion) while adjusting for covariates described above and as depicted in Table 1. Two sets of models were run, one with race and ethnicity and sex as main independent variables adjusting for study covariates, and the other with race and ethnicity and sex pair as the main independent variables adjusting for study covariates. As part of sensitivity analysis, we conducted regression analysis wherein the interaction term for race and ethnicity and sex was added as the main independent variable after controlling for study covariates. Further, we also ran analyses to examine changes in atrial fibrillation treatment across study years.
In all analyses, a two-sided P<0.05 was considered statistically significant. All analyses were conducted using R for Windows; version 4.0.2. The use of Optum was reviewed by the New England Institutional Review Board (IRB) and was determined to be exempt from broad IRB approval, as this research project did not involve active human subject participation.
Results
Baseline patient characteristics (Figure 1) depicts study attrition. Overall, the final cohort included 77,932 patients with incident AF. Baseline demographics of patients classified by race and ethnicity and sex are shown in Table 1. Mean age differed significantly across groups (P<0.001), where male patients were younger than female patients within each race group. The level of education also differed significantly across groups (P<0.001). Asian female (24.1%) and male patients (27.7%) had the highest rates of higher education (Bachelor’s or higher) among all races and ethnicities. A higher proportion of Black and Hispanic patients had ‘high school or less’ education, with Black female (47.7%) and Hispanic female patients (44.8%) having the highest rate among all groups. Risk factor and comorbidity burden also differed significantly across groups as evidenced by CHA2DS2VASc (P<0.001) and Elixhauser scores (P<0.001). Black and Hispanic female patients had the highest CHA2DS2VASc scores (4.3 ± 1.8) and Elixhauser scores (4.1 ± 2.8 and 4.0 ± 6.7, respectively) among all groups.
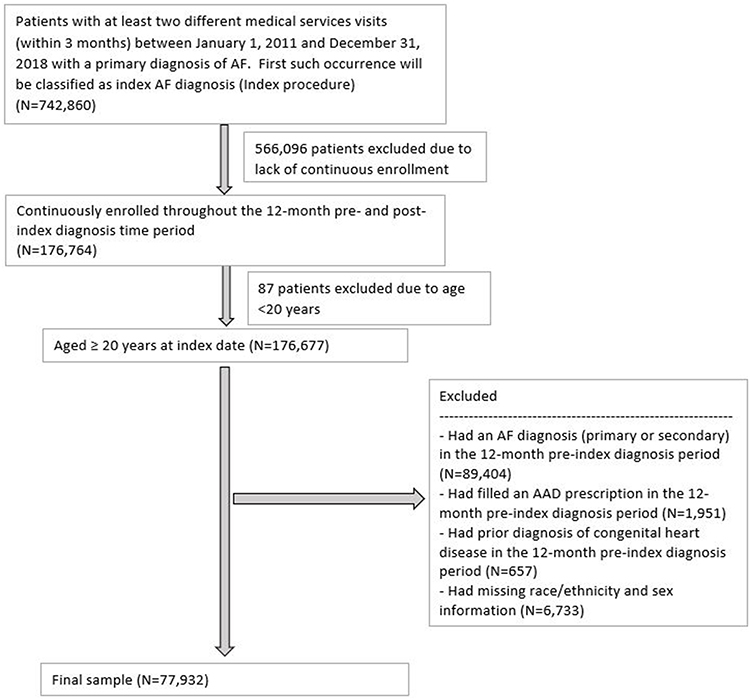 |
Figure 1 Sample attrition based on study inclusion and exclusion criteria. |
Association Between Race and Ethnicity and Sex and Rhythm Control Treatment for AF
Bivariate analysis showed significant differences in treatment rates by race and ethnicity and sex (Table 2). For AAD usage, White males (25.0%) were observed to have the highest rate, and Asian females (19.9%) had the lowest rate of AAD use within 1 year of incident AF diagnosis. For cardioversion, the rates were highest among White males (19.9%) and lowest among Asian females (8.1%). As per catheter ablation, White males (5.0%) had the highest rate with Hispanic females (2.3%) having the lowest rate. The rate of AF treatment was also observed to vary across study years (eTables 2–4). When examining the use of AADs (eTable 2), a significant decline in usage was observed for White males (26.82% in 2011 to 23.05% in 2019), White females (25.34% in 2011 to 19.03% in 2019), and Asian males (34.38% in 2011 to 22.08% in 2019) during the study period. In contrast, the rate of ablation (eTable 3) and cardioversion (eTable 4) seem to have improved during the study period. For example, for White males, the rate of ablation procedure increased from 3.43% in 2011 to 8.46% in 2019 (p<0.0001). Significant improvements in the rate of ablation procedure use was also observed for White females (1.64% in 2011 to 4.11% in 2019; p<0.0001), Black females (1.75% in 2011 to 4.72% in 2019; p=0.001), Asian males (6.25% in 2011 to 10.39% in 2019; p=0.005), Hispanic males (0.55% in 2011 to 5.67% in 2019; p=0.001), and Hispanic females (0.26% in 2011 to 5.41% in 2019; p=0.001) (eTable 3). As per cardioversion, significant improvements in use were seen for White males (16.17% in 2011 to 22.54% in 2019; p<0.0001) and White females (9.65% in 2011 to 15.63% in 2019; p<0.0001) during the study period, with no significant change observed for other race and ethnic and sex categories (eTable 4).
 |
Table 2 Bivariate Analysis Comparing Rhythm Control Treatment for Atrial Fibrillation by Race and Ethnicity and Sex |
Results from logistic regression analyses for receipt of each treatment by race and ethnicity (relative to White patients), sex (relative to males), and race and ethnicity-sex groups (relative to White males) are shown in Table 3. As stated earlier, we ran two models, with one model having race and ethnicity and sex as separate key independent variables of interest and the other having the merged variable as the key independent variable. Compared with White male patients, Black male patients (Odds ratio [OR] 0.72; 95% CI, 0.58–0.90) had significantly lower likelihood of receiving catheter ablation for AF within 1-year of incident AF diagnosis. Black male patients (OR 0.87; 95% CI, 0.79–0.96) were also less likely to initiate AAD, while Hispanic female patients (OR 1.17; 95% CI, 1.06–1.28) were more likely to initiate AAD, compared to White male patients. All groups were significantly less likely to undergo cardioversion compared to White males, with Asian female patients (OR 0.48; 95% CI, 0.37–0.63) having the lowest ORs. Results from sensitivity analysis with interaction term between race and ethnicity and sex showed similar results to the main analysis (eTables 5–7). For example, Black males were observed to have significantly lower likelihood of having an ablation as compared to White males (OR 0.72, 95% CI 0.58–0.89), similar to result from the main analysis.
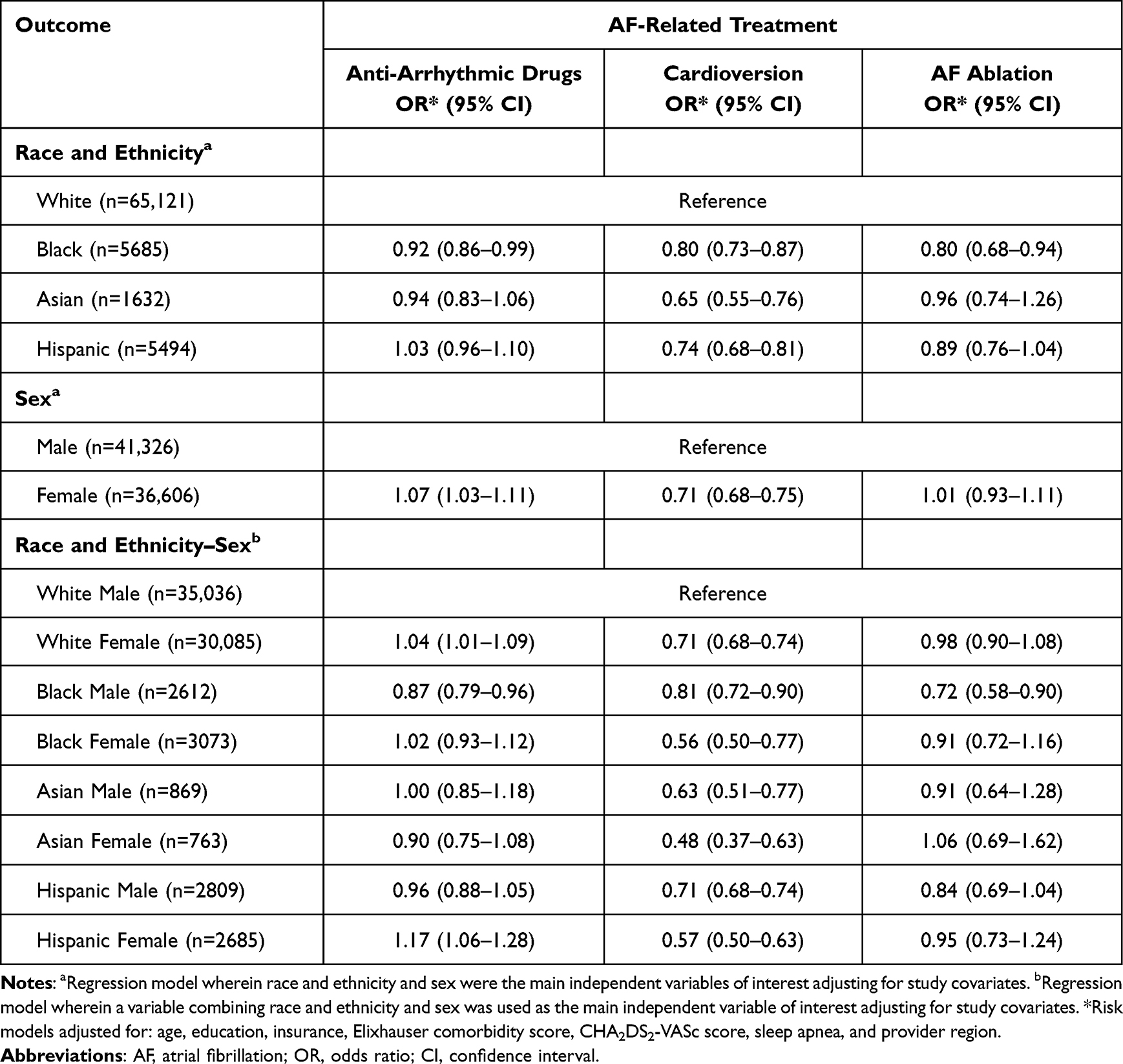 |
Table 3 Logistic Regression Model Results for Treatment of Incident Atrial Fibrillation by Race and Ethnicity, Sex, and Race and Ethnicity–Sex |
Discussion
In our analysis of nationwide outcomes data in more than 77,000 patients, we found several notable differences in management of AF by race, ethnicity, and sex. Compared with White male patients, Black male patients were less likely to undergo ablation and AAD treatment; and all other groups had significantly lower likelihood of undergoing cardioversion after AF diagnosis. The results suggest a lower utilization of rhythm control therapies, including the use of one or more AADs, catheter ablation, or cardioversion, in Black patients with AF. Notably, the underutilization was more prominent for ablation treatment compared to AAD or cardioversion treatment. Black males had 13% lower likelihood of receiving AAD treatment, 19% lower likelihood of receiving cardioversion, and 28% lower likelihood of receiving ablation treatment as compared to White males.
Prior research has demonstrated racial and sex differences in healthcare utilization for patients with AF.16,21–24 Several studies have also investigated the underlying differences among patients with AF.6–14,25–33 Naderi et al found that, compared to White male patients, Black male patients and other male patients from underrepresented racial and ethnic groups (UREGs) had 20–30% lower odds of catheter ablation; odds of catheter ablation were even lower among female patients regardless of race and ethnicity when compared to White male patients.10 In a study by Bhave et al, Black patients had lower likelihood of rhythm and rate control compared to White patients, and Hispanic patients had lower likelihood of catheter ablation.30 Our results align with those from these prior studies and build on those by integrating race and ethnicity and sex. As with prior research, we also observed Black patients to have lower likelihood of receiving AAD and catheter ablation treatment as compared to White patients (across both main analysis and sensitivity analysis). However, these differences primarily stemmed from the underutilization of these treatments among Black male patients. Though not approaching statistical significance, Black female patients were observed to have the lowest likelihood of receiving catheter ablation treatment among female patients, compared to White male patients, a trend that has been indicated in prior reports.10 Further, Hispanic females were observed to have higher utilization of AADs as compared to White male patients. These results suggest that there is considerable variation in rhythm control treatment among UREG patients, which necessitate assessment of AF management at the intersection of race and ethnicity and sex, rather than as separate components. To the best of our knowledge, this is the first study to examine the variation in AF treatment by intersection of race and ethnicity and sex.
Our analysis showed that Black and Hispanic female patients generally have the highest proportion of comorbid conditions associated with AF. These findings mirror previous analyses which demonstrated that both Black and Hispanic patients with AF had more traditional cardiovascular risk factors compared to White patients.33 Black and Hispanic female patients had the highest CHA2DS2VASc and Elixhauser scores, which increases the likelihood of stroke, heart failure, and/or death.28
In a sub-study from the Catheter Ablation and Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) trial, Thomas et al reported that catheter ablation was associated with significant reductions in primary endpoint of interest (a composite of all-cause mortality, disabling stroke, serious bleeding, or cardiac arrest; adjusted Hazard Ratio [aHR] 0.32; 95% CI 0.13–0.78) and AF recurrence (aHR 0.45; 95% CI 0.23–0.89) among racial and ethnic minorities.34 The reasons why racial and ethnic minority patients in the CABANA trial fared better with catheter ablation are complex and not fully understood. Irrespectively, the lower use of ablation among Black patients observed in our study remains concerning given the potential benefits of catheter ablation among UREGs with AF.
The underlying factors associated with underutilization of rhythm control strategies among UREGs are complex and warrant further investigation. These factors potentially include clinical appropriateness, barriers to healthcare access, lack of proper training and resources among physicians, patient preferences in treatment and healthcare use, conscious or unconscious bias among physicians, and low health literacy among patients which impedes informed decision-making. Low health literacy could preclude patients from fully understanding the disease burden presented by AF or the risk and benefits of procedural therapy. Though all patients in our study had healthcare insurance, there could be variation in geographic and economic access to health services, which could have contributed to lower treatment among UREGs with AF. Physician training and access to resources in treating UREG patients presenting with AF symptoms could influence treatment. In their study of medical evaluation and management of Medicare beneficiaries, Bach et al found that primary care physicians treating Black patients versus White patients were less likely to be board certified and more likely to report access barriers in terms of providing quality care to their patients.35 Patient preferences are a critical component of treatment uptake. Several studies have suggested higher rates of refusal for cardiovascular procedures among Black and female patients.36–39 Future research should be aimed at understanding the drivers of patient preference as well as impact of social determinants of health in UREGs with AF and how these determinants may affect uptake of rhythm control therapies. Additionally, qualitative inquiry, specifically mixed method approaches, are needed to better understand barriers and facilitators to the uptake of rhythm control strategies for treatment of AF.
Limitations
Given that this analysis is retrospective in nature, we cannot exclude the possibility of residual confounding. Several factors that affect treatment decisions such as prognostic indicators or disease severity were not available (eg, left atrial volume index, AF burden). Other factors such as patient preference, patient income,15 physician specialty, and physician experience could potentially have influenced treatment for AF, were also not included in the study. Coding errors during claims processing can affect identification of services and subsequently the results of this analysis. However, there is no reason to expect variation in coding errors by race or sex. Given the differential use of medical services for treatment of AF by race, ethnicity, and sex, we cannot exclude the potential for diagnostic bias for the detection of AF between races and sexes. There was a disproportionate representation of patients with AF by race, ethnicity, and sex in our study. Further, the patients in Optum database, used in this study, are enrollees of United Healthcare commercial and Medicare Advantage insurance plans. As such, our results may not be generalizable to patients with non-commercial insurance including self-pay, Medicaid, and Medicare fee-for-service insurance.
Conclusions
Using data from a large private health insurance dataset, this study identified differences in the treatment of AF by race, ethnicity, and sex. Rhythm control strategies were used less in Black patients, particularly in Black male patients. Further research is warranted for a better understanding of the causes of racial, ethnic, and sex differences in the rhythm treatment of AF.
Abbreviations
AAD, antiarrhythmic drug; AF, atrial fibrillation; ICD-9, International Classification of Diseases, Ninth Revision; ICD-10, International Classification of Diseases, Tenth Revision; UREG, underrepresented racial and ethnic group.
Funding
This work is supported by Johnson & Johnson.
Disclosure
Diane M Francis, Sonia Maccioni, Vincent C Thomas, Paul Coplan, Rahul Khanna, Charlene Wong, and Neloufar Rahai are Johnson & Johnson employees. Dr Larry R Jackson II has received: research grants from the National Institute of Health, specifically the National Institute on Minority Health and Health Disparities. Dr Jackson is currently supported by 1K01HL159041 from the National Heart, Lung and Blood Institute and the American Association under award number 851386 and serves as a consultant to Biosense Webster, Johnson & Johnson, Sanofi, Bristol Myers Squibb and Pfizer and receives honoraria from Zoll LifeVest, CME outfitters, Health Monitor, PRIME Education, and WebMD/Medscape. Dr Friedman has received research grants from the American Heart Association, National Cardiovascular Data Registry, Boston Scientific, Abbott, Medtronic, Merit Medical, and Biosense Webster and consulting fees from Abbott, AtriCure, and Sanofi. Dr Jonathan P Piccini is supported by R01HL128595 from the National Heart, Lung and Blood Institute and receives grants for clinical research from Abbott, American Heart Association, Association for the Advancement of Medical Instrumentation, Bayer, Boston Scientific, National Institutes of Health, and Philips and serves as a consultant to Abbott, AbbVie, Ablacon, Altathera, ARCA Biopharma, Biotronik, Boston Scientific, Bristol Myers Squibb, LivaNova, Medtronic, Milestone, ElectroPhysiology Frontiers, Itamar, Pfizer, Sanofi, Philips, ResMed, and Up-to-Date. The authors report no other conflicts of interest in this work.
References
1. Wyndham CR. Atrial fibrillation: the most common arrhythmia. Tex Heart Inst J. 2000;27:257–267.
2. Kornej J, Börschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century. Circ Res. 2020;127:4–20. doi:10.1161/circresaha.120.316340
3. Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. doi:10.1161/circulationaha.105.595140
4. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults. JAMA. 2001:285. doi:10.1001/jama.285.18.2370
5. Kirchhof P, Camm AJ, Goette A, et al. Early rhythm-control therapy in patients with atrial fibrillation. New Engl J of Med. 2020;383:1305–1316. doi:10.1056/NEJMoa2019422
6. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125–e151. doi:10.1161/CIR.0000000000000665
7. Bukari A, Nayak H, Aziz Z, Deshmukh A, Tung R, Ozcan C. Impact of race and gender on clinical outcomes of catheter ablation in patients with atrial fibrillation. Pacing Clin Electrophysiol. 2017;40:1073–1079. doi:10.1111/pace.13165
8. Patel N, Deshmukh A, Thakkar B, et al. Gender, race, and health insurance status in patients undergoing catheter ablation for atrial fibrillation. Am J Cardiol. 2016;117:1117–1126. doi:10.1016/j.amjcard.2016.01.040
9. Kummer BR, Bhave PD, Merkler AE, Gialdini G, Okin PM, Kamel H. Demographic differences in catheter ablation after hospital presentation with symptomatic atrial fibrillation. J Am Heart Assoc. 2015;4:e002097. doi:10.1161/jaha.115.002097
10. Cheng X, Hu Q, Gao L, Liu J, Qin S, Zhang D. Sex-related differences in catheter ablation of atrial fibrillation: a systematic review and meta-analysis. Europace. 2019;21:1509–1518. doi:10.1093/europace/euz179
11. Kaiser DW, Fan J, Schmitt S, et al. Gender differences in clinical outcomes after catheter ablation of atrial fibrillation. JACC Clin Electrophysiol. 2016;2:703–710. doi:10.1016/j.jacep.2016.04.014
12. Weberndorfer V, Beinart R, Ricciardi D, et al. Sex differences in rate and rhythm control for atrial fibrillation. Europace. 2019;21:690–697. doi:10.1093/europace/euy295
13. Avgil Tsadok M, Gagnon J, Joza J, et al. Temporal trends and sex differences in pulmonary vein isolation for patients with atrial fibrillation. Heart Rhythm. 2015;12:1979–1986. doi:10.1016/j.hrthm.2015.06.029
14. Beck H, Curtis AB. Sex differences in outcomes of ablation of atrial fibrillation. J Atr Fibrillation. 2014;6:1024. doi:10.4022/jafib.1024
15. Eberly LA, Garg L, Yang L, et al. Racial/ethnic and socioeconomic disparities in management of incident paroxysmal atrial fibrillation. JAMA Netw Open. 2021;4:e210247. doi:10.1001/jamanetworkopen.2021.0247
16. Fiscella K, Franks P, Gold MR, Clancy CM. Inequality in Quality. JAMA. 2000;283(19):2579. doi:10.1001/jama.283.19.2579
17. Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27. doi:10.1097/00005650-199801000-00004
18. Chen PC, Lip GY, Yeh G, Lin HJ, Chien KL. Risk of bleeding and stroke with oral anticoagulation and antiplatelet therapy in patients with atrial fibrillation in Taiwan: a nationwide cohort study. PLoS One. 2015;10:e0125257. doi:10.1371/journal.pone.0125257
19. Friedman DJ, Pokorney SD, Ghanem A, et al. Predictors of cardiac perforation with catheter ablation of atrial fibrillation. JACC Clin Electrophysiol. 2020;6:636–645. doi:10.1016/j.jacep.2020.01.011
20. Friedman DJ, Field ME, Rahman M, et al. Catheter ablation and healthcare utilization and cost among patients with paroxysmal versus persistent atrial fibrillation. Heart Rhythm O2. 2021;2:28–36. doi:10.1016/j.hroo.2020.12.017
21. Williams DR, Rucker TD. Understanding and addressing racial disparities in health care. Health Care Financ Rev. 2000;21:75–90.
22. Fiscella K, Franks P, Doescher MP, Saver BG. Disparities in health care by race, ethnicity, and language among the insured: findings from a national sample. Med Care. 2002;40:52–59. doi:10.1097/00005650-200201000-00007
23. Kent JA, Patel V, Varela NA. Gender disparities in health care. Mt Sinai J of Med. 2012;79:555–559. doi:10.1002/msj.21336
24. Manuel JI. Racial/ethnic and gender disparities in health care use and access. Health Serv Res. 2018;53:1407–1429. doi:10.1111/1475-6773.12705
25. Bhatia S, Qazi M, Erande A, et al. Racial differences in the prevalence and outcomes of atrial fibrillation in patients hospitalized with heart failure. Am J Cardiol. 2016;117:1468–1473. doi:10.1016/j.amjcard.2016.02.016
26. Hoyt H, Nazarian S, Alhumaid F, et al. Demographic profile of patients undergoing catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2011;22:994–998. doi:10.1111/j.1540-8167.2011.02043.x
27. Tamariz L, Rodriguez A, Palacio A, Li H, Myerburg R. Racial disparities in the use of catheter ablation for atrial fibrillation and flutter. Clin Cardiol. 2014;37:733–737. doi:10.1002/clc.22330
28. Nanda A, Kabra R. Racial differences in atrial fibrillation epidemiology, management, and outcomes. Curr Treat Options Cardiovasc Med. 2019;21:85. doi:10.1007/s11936-019-0793-5
29. Freeman JV, Tabada GH, Reynolds K, et al. Contemporary procedural complications, hospitalizations, and emergency visits after catheter ablation for atrial fibrillation. Am J Cardiol. 2018;121:602–608. doi:10.1016/j.amjcard.2017.11.034
30. Bhave PD, Lu X, Girotra S, Kamel H, Vaughan Sarrazin MS. Race- and sex-related differences in care for patients newly diagnosed with atrial fibrillation. Heart Rhythm. 2015;12:1406–1412. doi:10.1016/j.hrthm.2015.03.031
31. Magnussen C, Niiranen TJ, Ojeda FM, et al. Sex differences and similarities in atrial fibrillation epidemiology, risk factors, and mortality in community cohorts: results from the BiomarCaRE consortium (biomarker for cardiovascular risk assessment in Europe). Circulation. 2017;136:1588–1597. doi:10.1161/circulationaha.117.028981
32. Mou L, Norby FL, Chen LY, et al. Lifetime risk of atrial fibrillation by race and socioeconomic status: ARIC study (atherosclerosis risk in communities). Circ Arrhythm Electrophysiol. 2018;11:e006350. doi:10.1161/circep.118.006350
33. Golwala H, Jackson LR 2nd, Simon DN, et al. Racial/ethnic differences in atrial fibrillation symptoms, treatment patterns, and outcomes: insights from outcomes registry for better informed treatment for atrial fibrillation registry. Am Heart J. 2016;174:29–36. doi:10.1016/j.ahj.2015.10.028
34. Thomas KL, Al-Khalidi HR, Silverstein AP, et al. Ablation versus Drug Therapy for Atrial Fibrillation in Racial and Ethnic Minorities. J Am Coll Cardiol. 2021; 78(2):126–138. doi:10.1016/j.jacc.2021.04.092
35. Bach PB, Pham HH, Schrag D, Tate RC, Hargraves JL. Primary Care Physicians Who Treat Blacks and Whites. N Engl J Med. 2004;351(6):575–584. doi:10.1056/NEJMsa040609
36. Heidenreich PA, Shlipak MG, Geppert J, McClellan M. Racial and sex differences in refusal of coronary angiography. Am J Med. 2002;113(3):200–207. doi:10.1016/S0002-9343(02)01221-4
37. Maynard C, Fisher LD, Passamani ER, Pullum T. Blacks in the coronary artery surgery study (CASS): race and clinical decision making. Am J Public Health. 1986;76(12):1446–1448. doi:10.2105/AJPH.76.12.1446
38. Rathore SS, Ordin DL, Krumholz HM. Race and sex differences in the refusal of cardiac catheterization among elderly patients hospitalized with acute myocardial infarction. Am Heart J. 2002;144(6):1052–1056. doi:10.1067/mhj.2002.126122
39. Whittle J, Conigliaro J, Good C, Joswiak M. Do Patient Preferences Contribute to Racial Differences in Cardiovascular Procedure Use?. J Gen Intern Med. 1997;12(5):267–273. doi:10.1046/j.1525-1497.1997.012005267.x
[ad_2]
Source link