[ad_1]
Introduction
In the United States, the intersection of social determinants of health, underscores the heightened susceptibility of individuals racialized as Black to Alzheimer’s disease (AD), with projections indicating a two to four times higher risk compared to their racialized White counterparts.1,2 Black individuals are also more likely to develop mild cognitive impairment, which often progresses to a diagnosis of Alzheimer’s disease.2–5 Additionally, Black individuals frequently receive a diagnosis of dementia at more advanced disease stages.6 Previous studies emphasize the notable lack of representation of Black adults in clinical trials for dementia.7,8 The increased prevalence of dementia within the Black community accentuates the pressing need to rectify the inadequacy in recruiting this demographic in clinical trials.
Several factors contribute to the greater participation of White individuals enrolled in clinical trials compared to their Black counterparts. These factors find their roots in historical, socio-economic, and systemic disparities that persist today. Notably, the infamous Tuskegee Syphilis study, stands as a poignant example of unethical practices, with the deliberate withholding of syphilis treatment from Black men, leading to severe harm and fostering mistrust among Black individuals.9 Contemporary influences on this ongoing disparity encompass a range of dimensions, including negative attitudes, limited awareness of clinical trials, religious beliefs, and enduring systemic and structural challenges, such as restricted access to transportation, insurance coverage, and high-quality healthcare.10
Underrepresentation of Black participants is evident in various clinical trial scenarios. Notable instances, include breast cancer trials where Black women are underrepresented despite experiencing higher mortality rates.11 Additionally, cardiovascular trials, specifically heart failure trials, often exhibit limitation in evaluating the efficacy and safety of new medications and treatments within the Black population.12
The purpose of this paper is to present information on the challenges and successes in recruiting Black individuals into the I-CONECT clinical trial which is a behavioral intervention for older old (age 80 and above) adults with and without mild cognitive impairment (MCI).13 The objectives include: 1) Describe the lessons learned while recruiting socially isolated and lonely Black participants aged 80 and older into a behavioral intervention trial where information and communication technology was used as a tool to enhance cognitive reserve, 2) Compare participation rates between Black and White individuals, and 3) Discuss factors that lead to higher enrollment rates among Black participants for use in future trials.
Materials and Methods
Background
The I-CONECT study is a multi-site randomized controlled behavioral intervention trial (ClinicalTrial.gov: NCT02871921). The study protocol and its rationale are described elsewhere.13,14 The I-CONECT study was developed to provide easy-to-start behavioral interventions that could be delivered to older old, socially isolated individuals with low motivation or who are homebound. The initial target population encompassed individuals aged 80 and over, both Black and White, who exhibited social isolation or reported subjective loneliness. Box 1 provides detailed inclusion and exclusion criteria for the study.
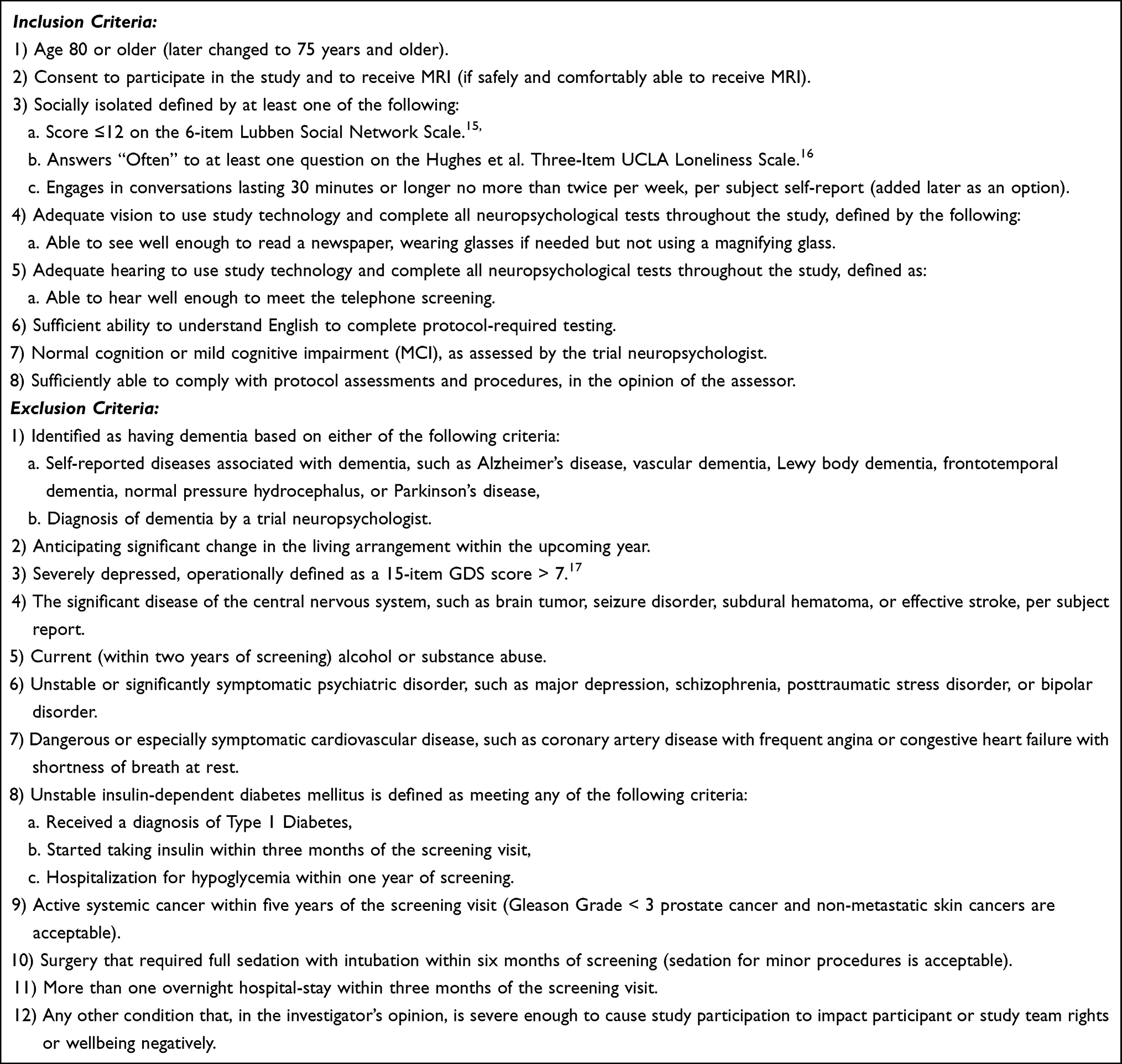 |
Box 1 Overall Recruitment Statistics for the Two Study Sites |
A consensus meeting was convened with the study’s team of neurologists and neuropsychologists to assess the cognitive status grouping (Normal Cognition, MCI or Dementia) of each prospective participant, utilizing a standardized methodology consistent with that employed in the National Institute of Health(NIH)-funded Alzheimer’s Disease Centers across the United States.18–20 Individuals diagnosed with dementia were subsequently excluded from the study. Participants were randomized into either control or intervention groups within each diagnostic group.
Participants in the intervention group were provided with computer and internet access video chat with trained staff, initially engaging for 30 minutes per day, four days per week for six months, followed by twice a week for another six months. A device that is easy for older adults was designed to streamline the process. Both control and experimental groups had a 10-minute weekly telephone check-in to monitor social activities and enhance retention. Monetary incentives included $50 to $100 for testing throughout the study, carefully set to avoid undue inducement while allowing participants to maintain income assistance. The Institutional Review Board approved the study at the primary Pacific Coast site (IRB Study 0015937). All participants were required to provide written informed consent and were included in the analysis (experimental and control groups). The study was conducted in compliance with the ethical principles of the Declaration of Helsinki.
Population
We aimed to recruit 160 Black and 160 White participants, including an equal number of those with normal cognition and MCI. The primary study site situated on the US Pacific coast, had limited Black representation. To address this and meet our recruitment targets, we established a secondary study site in a US Midwest region recognized for its significant Black population. It is important to note that no Black potential subjects were recruited from the US Pacific coast, and there was no attempt to recruit White individuals from the Midwest site.
Initial Recruitment Strategies
The Minority Recruitment Model enhanced recruitment.21,22 It was created by social scientists for older ethnic minority individuals requiring a balance between the research team’s needs and the community’s perspectives on research. The premise of the model is that the decision-making process leading individuals to participate or refuse participation in research is influenced by the social context of research participants and their community agencies, as well as that of the researchers and their institutions.
The above Minority Recruitment Model21,22 and best practices for reaching Black individuals were planned to recruit and retain participants in this study.23–26 We hired a Black study coordinator who was culturally sensitive to the older old Black population and who knew the urban areas where the recruitment efforts would occur. Research staff was trained to work with older adults with the expectation that they may need to make multiple phone calls and repeat information several times due to age-related changes, especially for those with MCI. Every effort was made for the same research staff member to conduct all the home visits and follow-up phone calls for each participant.
Recruitment materials were developed explicitly for the Black potential participants with input from the study coordinator and older Black adult volunteers. The booklet was designed to show pictures of Black older adults participating in computer-related activities. Content used large print and bullet points with clear short statements explaining the study to offset any biases and age-related physiological changes.
In our study, we had initially planned to employ a recruitment strategy involving collaboration with Meals on Wheels, a non-profit organization dedicated to delivering meals to economically disadvantaged or home-bound older individuals, as well as the Area Agency on Aging (AAA), which offers a range of services. While this recruitment approach was successfully implemented at our Pacific coast site, where study personnel actively participated in meal delivery, it faced challenges at our Midwest site. Despite multiple meetings and discussion, we encountered limitations that restricted our engagement to a brief period of flyer distribution.
In the pursuit of building trust and garnering valuable insights from the community for our research endeavors, the Healthy Black Elders (HBE) community-based program, a well-established and reputable research partnership, was one of the primary recruitment sources.27 This initiative adheres to the fundamental principles of community-based participatory research (CBPR), a collaborative approach between academic researchers and community members. The approval process for this research study, which sought access to the research list of potential participants, was both comprehensive and collaborative in nature. It encompassed several key stages, starting with a community board meeting to deliberate the research proposal, an ethical review with particular focus on safeguarding informed consent and respecting the rights of participants. Furthermore, careful scrutiny was given to the alignment of the study with distinctive health concerns and priorities of the community it aimed to serve.
An additional key recruitment source employed in our study was the election list, which supplied us with names and addresses of individuals residing in our designated urban areas with the Midwest region. To leverage this resource, we distributed study material via mail, with the sole option for potential participants being to send back a prepaid op-in-card, indicating their consent to be contacted by our research staff. It is noteworthy that, in contrast, the Pacific site had the opportunity to send prepaid opt-out materials, allowing potential subjects to return an opt-out card. Pacific research staff would then call the potential participant one week after mailing the materials, if they did not receive the op-out-card.
Other recruitment strategies used and widely suggested in the literature as essential for older Black participants included attendance at health fairs and contacts through networks of friends, family, and churches.24,26 Additionally, recruitment efforts were bolstered through the utilization of the www.I-CONECT.org study website, write-ups in community newsletters, social media postings, and online advertisements (Twitter and Facebook). It is worth noting that due to the variances in state regulations and agency requirements to allow access to older Black individuals, a second full-time Black recruitment coordinator was hired to engage with community groups.
Recruitment Data Collection
Recruitment data was collected using Research Electronic Data Capture (REDCap), a web-based application that captures clinical research data, is HIPAA compliant, and is highly secure. The descriptive data collected in the study included the number of contacts needed to recruit participants (including mass mailing), the number who agreed to the phone screening, the number of home visits completed before randomization, and the number of participants who dropped out between randomization and the start of the intervention. Data was also collected on the number and reasons for screening failures after the first home visit, which included the assessment of neuropsychological tests, social isolation scores, or other measurements used to determine eligibility for inclusion and exclusion criteria. We compared screening failures and their reasons between the two sites and overall participation and eligibility rates between Black and White participants. Descriptive data on the best strategies to recruit Black participants for screening and enrolling participants in the study were tabulated.
Revised Recruitment Procedures
Changes in Eligibility Criteria
Once the study was underway, our initial inclusion criteria created challenges in recruiting older Black individuals. We found that potential participants over 80 were difficult to find. The initial age criterion was set from the literature defining “older old”, which drew from studies containing White participants.28,29 Given the reduced life expectancy of the US Black population compared to the White population now estimated at 4.7 years,30 we lowered the age criterion to 75 years and older to provide a cohort with similar life phases.
Also, we found that older urban Black individuals were less likely than White individuals to live alone, which was an initial inclusion criterion of social isolation.31 The criterion was changed so that all participants who lived with someone could participate if they met at least one other social isolation criterion. The defining criteria of social isolation were amended to include an additional option of engaging in conversations lasting 30 minutes or longer, no more than twice per week, per subject self-report, which was more aligned with the social communication patterns of the target population of older old Black. We also found that family member participation in the consenting process was beneficial because of the proximity to family members. The family members’ understanding of the participant allowed better communication of the study protocol before consent.
Additional Protocol Changes
During the consenting process, several potential Black potential participants were concerned about giving a saliva sample for genotype (for information on APOE 4) due to the fear and mistrust that their DNA would be used in different ways without their consent. The protocol was then changed to allow participants to opt out of giving saliva samples if the participant chose to do so. Also, the initial protocol requiring some participants to have two magnetic resonance imaging (MRI) studies were changed from required to voluntary participation. The travel, participation time, and the claustrophobia of the MRI procedure caused several Black participants to decline the procedure.
Results
Comparing Recruitment Numbers Between the Two Study Sites
Significant effort was made to contact potential participants via mass mailings, advertisements, and direct community outreach. While both study sites had approximately the same recruitment budget, the Midwestern site, recruiting Black individuals, enrolled fewer participants. Table 1 describes the proportion of participants remaining in the participant pool through each phase of determining eligibility for study enrollment. The primary Pacific Coast site contacted 17,523 potential participants and enrolled/randomized 145 White and 2 Asian/mixed race participants (0.8%). The Midwestern site contacted 12,141 Black potential participants and enrolled/randomized 39 (0.3%) participants.
 |
Table 1 Overall Recruitment Statistics for the Two Study Sites |
Recruitment Sources for Black/African American Participants
Table 2 describes the recruitment sources and their respective participant yield and success rate for the Midwest study site. The recruitment source that provided the highest number of telephone screening contacts was the Healthier Black Elders Registry (HBE) mailings (N=208, 49% of telephone screened), where potential participants could call back and ask about the study. The second telephone screening recruitment source was the election voting list mailings in targeted areas (N=121, 28.3% of telephone screened). Various other sources yielded smaller recruitment numbers including word of mouth, fliers, public outreach (N=47, 11% of telephone screened), and finally, community outreach senior housing (N=19, 4.4% of telephone screened).
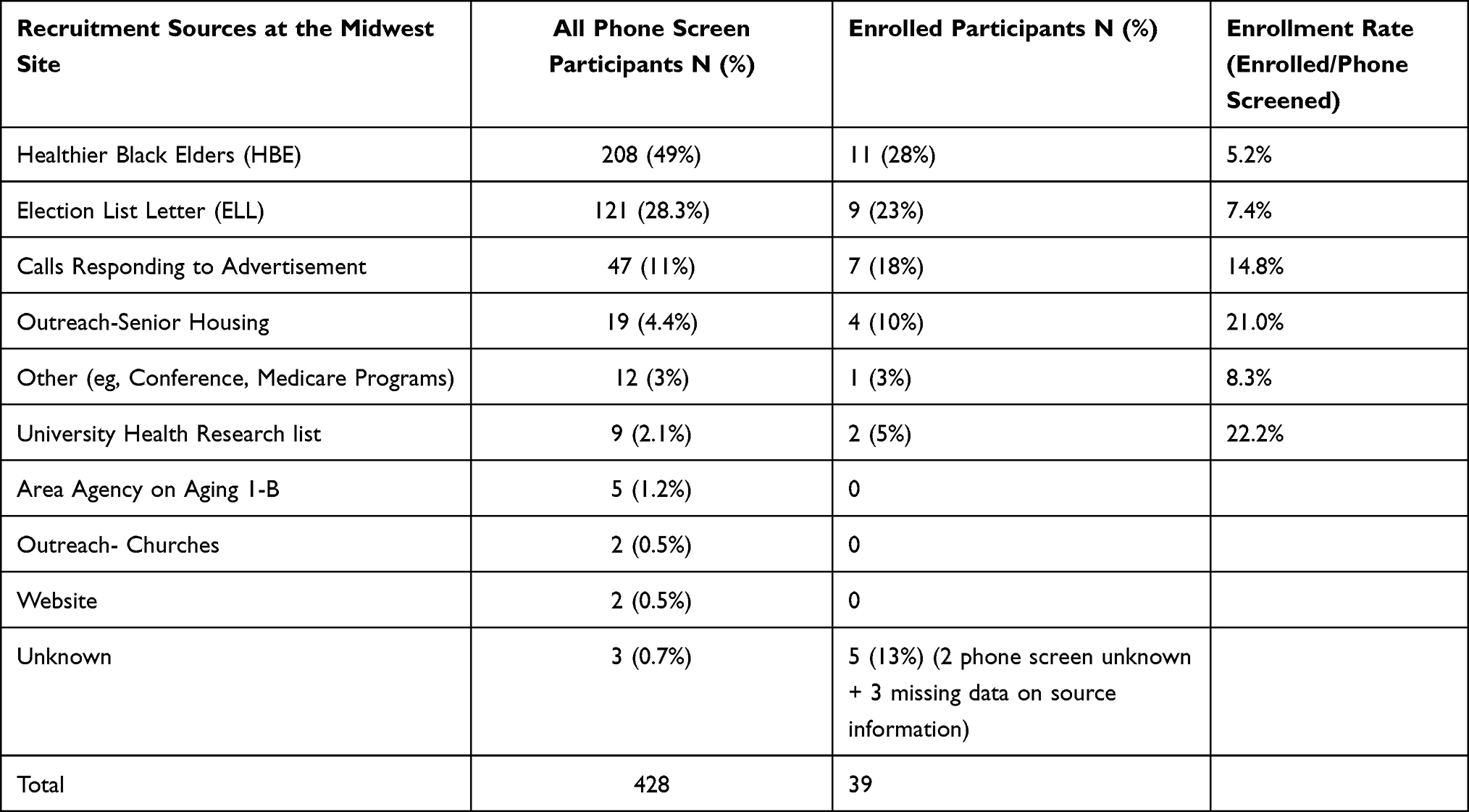 |
Table 2 Recruitment Sources for Black Participants at Midwest Site |
The top sources that successfully enrolled Black participants in the study were the HBE (N=11, 28%), election list (N=9, 23%), advertisement calls (N=7, 18%), and senior outreach housing (N=4,10%). However, in terms of the rate of enrolment from the total number of telephone screenings, the election voting list mailings in targeted areas had the highest rate. The sources that did not yield enough participants included the Area Agency on Aging, churches, and websites.
Retention of Participants Through All Study Phases
Figure 1 illustrates the many process steps from telephone screen to enrolment/randomization, at which point the study started for each participant. Out of the 428 Black/African American potential participants who were telephone screened, 274 (63%) met the revised age criteria (≧75). Among 274 potential participants who met the age criteria, 120 (42.8%) completed at least one revised social isolation criterion. Among these 120 potential participants, 65 (54.2%) were excluded due to health conditions. Please refer to the Box for details on inclusion and exclusion criteria. The remaining 55 (12.8%) out of the 428 potential participants who telephone screened consented to a home screen in-person visit. Among the White participants who were telephone screened (N=711), 702 (98.7%) potential participants met the age criteria, and 378 potential participants 53 (8%), completed at least one of the social isolation criteria. Among 378 potential participants, 169 (44.4%) were excluded due to health conditions, and the remaining 210 (29.5%) consented to a home screen.
 |
Figure 1 Recruitment Flow Comparison. This figure illustrates the recruitment process, comparing potential participants from the Midwest site (Black older adults) and the Pacific Coast (White older adults). The flow chart outlines the following stages: 1. Initial Contact: The initial contact was made with potential participants. 2. Telephone Screen Agreement: Basic eligibility is assessed and if criteria are met, a home visit is scheduled. 3. Home Visit with Consent and Screen: Eligible participants undergo a home visit for obtaining consent and further screening. 4. Number of Screen Failures: This indicates the count of participants who did not meet the screening process. 5. Randomization: Participants are randomly assigned to experimental and control groups. 6. Withdrawal Before the Trial: The number of participants who withdrew before the trial commences is shown. 7. Trial Start: The figure compares the participants who started the trial for the experimental and control groups for each site. |
Table 3 describes reasons for screening failures during the in-home assessments, including health indicators and neuropsychiatric screenings. The primary cause of screen failures during the baseline home visit at both sites was participants no longer meeting the updated isolation criteria (27.6% for Blacks and 35.9% for Whites), despite having initially met the criteria during telephone screening. Various factors may have played a role in this, including elapsed time between telephone screening and the baseline visits, incorporation of revised isolation criteria, which encompassed three distinct criteria and the potential shifts in participants’ levels of social isolation. Furthermore, Black participants had a higher rate (27.6%) of difficulty in continuing protocol assessments due to anticipated changes in living arrangements, time commitments, and recent medical issues than White participants (9.4%). Another reason for home visit screen failures was participants were diagnosed with dementia by consensus with the Neuropsychologist and Neurologist (Blacks 13.8% and Whites 9.4%). None of the participants had vision difficulties, and only one Black participant had significant hearing loss that precluded participation despite the use of hearing aids. Interestingly, during the screening/baseline visit, when the participant met study staff in their home, all the Black participants agreed to continue, but 6 (9.4%) White participants declined to continue when the study was explained.
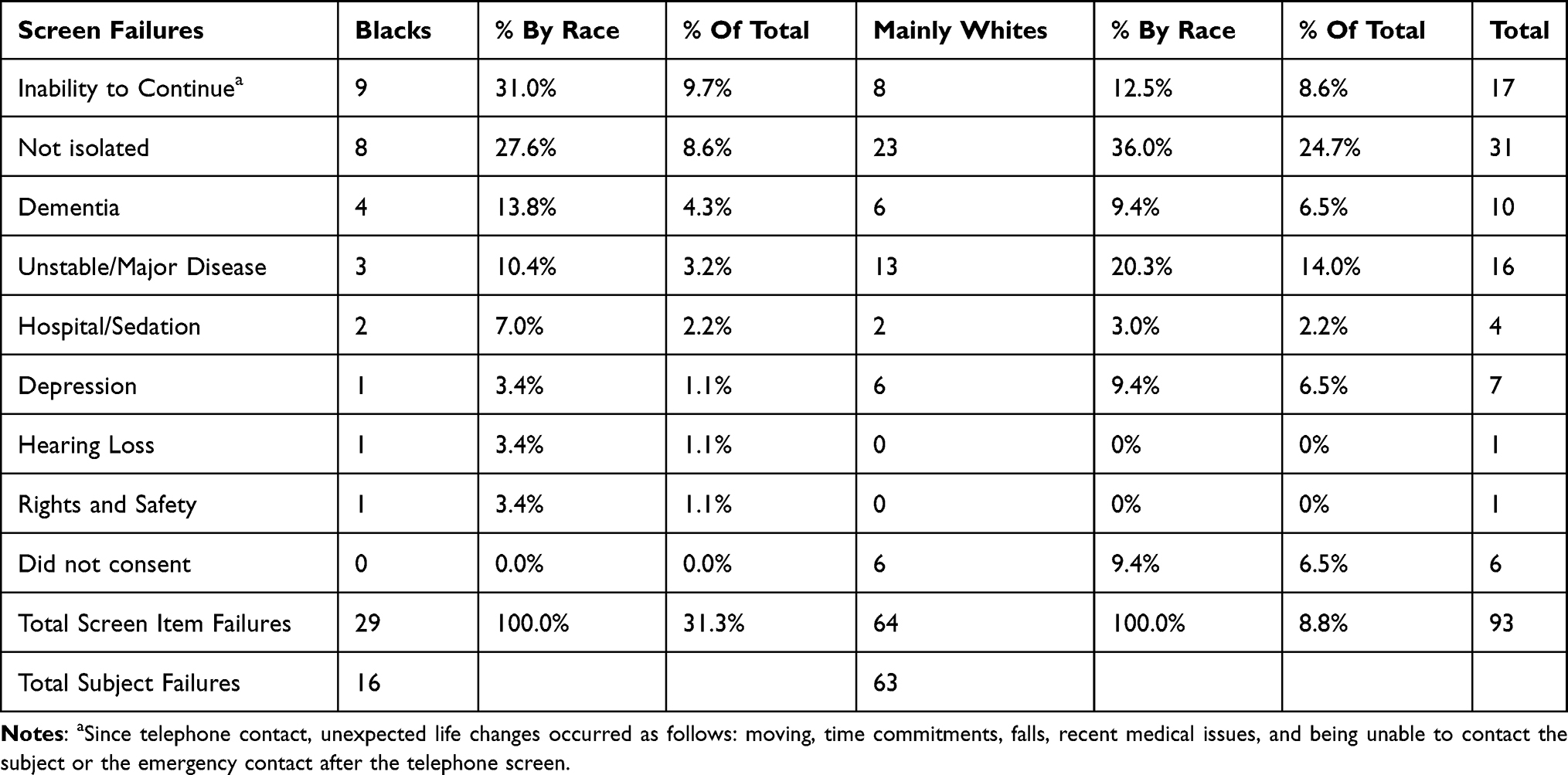 |
Table 3 Reasons for Screen Failures During in-Home Screening for the Two Study Sites |
Once the study began, dropout rates differed between the two study sites. Half of the Black participants, who consented and then randomized into the experimental group dropped out before the initiation of the trial. The reasons given were time commitment (N=3), internet connection issues (N =2), surgery (N =1), work/ family commitments (N=2), and not being interested after COVID delayed the study for three months (N=3). None of the Black participants in the control group dropped out. For White participants, 15 (20%) dropped out of the intervention group, and 6 (8%) dropped out of the control group after randomization but before the initiation of the trial.
Discussion
The Minority Recruitment Model Recruitment Model21,22 identified barriers based on factors at the individual, community, and research community levels. Our initial recruitment efforts used best practices for recruiting Black/ participants into research studies, including health fairs, friend and family networks, and churches.23–26 Despite these efforts, we encountered challenges in reaching a specific demographic; socially isolated, older Black individuals residing in urban areas. Our recruitment rates for this population were impacted by multiple factors, including recruitment criterion measurement that required amendment for both sites, distinct regional regulations, variations in institutional policies, diverse community preferences, and varying ethical considerations, particularly in relation to participants in the Meals on Wheels and Area Agency on Aging initiatives at the two study sites, along with the utilization of opt-in and opt-out methodologies. Furthermore, the study population were older who may have MCI, the complexity of the study, lack of family involvement and underestimation of the magnitude of effort and cost required to recruit a large sample using multiple methods, each with small yields. Additionally, the COVID-19 pandemic reduced the recruitment and retention of Black/African American participants.
Lowering the age criterion to 75 years and over, enhanced our recruitment efforts especially for Black participants. Isolation and loneliness inclusion criteria may have incorrectly assumed that older Black individuals have a similar way of living in social isolation as Whites. Yet, a recent study found that Whites are more likely to live alone, be childless, and have limited contact with religious congregation members than Blacks.31 Another study characterized personal and neighborhood contextual influences on social isolation and loneliness and found that Blacks were less likely to report social isolation or loneliness and did not live alone.32 Older Black individuals are more likely to be involved with family and play a significant role in helping grandchildren or have an adult child or other family members living with them.31 This lower prevalence of what is traditionally thought of as social isolation posed more challenges in our recruitment of older old Black individuals.
Research on social isolation and loneliness has historically focused on White populations. The scientific community needs to better understand social isolation within diverse cultural communities. Since the experience of loneliness and social isolation are culturally influenced, measurement must be relative to the social norms influencing that experience.33 Removing the requirement that participants live alone to be “socially isolated” and the amendment of the defining criteria of social isolation to include engaging in conversations lasting 30 minutes or longer, no more than twice per week, per subject self-report, was more aligned with the social communication patterns of the older old Black individuals and enhanced recruitment. Cultural norms, values, and family dynamics can be shaped by experiences of loneliness and isolation. Older Black individuals often have strong family and community connections. The nature of these relationships and the role of family support can influence feelings of loneliness and isolation requires further study.
The Healthy Black Elders community-based program yielded the most significant percentage of screened participants (28.3%), which was far lower than the anticipated number. Healthy Black Elders is a research collaborative registry of older Black adults.27 Yet those who responded through the HBE with interest in participating in the study had high social engagement and interactions. Thus, many were not eligible for our research. Our second most significant yield (49% of screened contacts) was a novel approach of mass mailings to targeted zip codes with a high proportion of Black residents. This required sending thousands of mailings to yield 121 potential subjects who then called us and were screened for the study.
Incorporating a more formalized family involvement approach into the decision-making process for study consent has the potential to significantly enhance recruitment efforts. Frequently, potential older Black participants, upon being apprised of the study details, expressed a desire to consult with their family first before giving consent. This inclination aligns with the deep-rooted cultural values of strong family bonds, interdependence, and support networks prevalent in many communities. Notably, while a dementia diagnosis is an exclusion criterion, the study encompasses older adults both with and without MCI, who may find solace in the presence of a trusted family member when deciding to engage in research.
To optimize recruitment, it is imperative to design advertisements, outreach strategies, and study materials aimed at educating and informing potential participants as well as those who wield influence in the life of the potential participant. Implementing protocols that facilitate the active involvement of family/trusted friend, offering frequent opportunities to pose clarifying questions and delivering crucial trial information in a staggered reiterated manner, holds promise for increasing participant recruitment. This approach can also alleviate concerns among family members who might otherwise dissuade the person from study participation due to lack of understanding about the research or unanswered questions.34
Furthermore, it is essential to consider the influence of cultural beliefs on the willingness of older Black individuals to engage in a clinical trial related to cognitive health. In some instance, these participants may perceive memory loss or cognitive issues as natural consequences of aging and exhibit reluctance to participate in research aimed at delaying the onset of dementia.35 Additionally, the prospect of labelling individuals specifically with MCI may potentially hinder recruitment efforts by introducing negative social and emotional implications. To address these issues, it is recommended to provide culturally relevant education and information about cognitive health and engage in discussion that acknowledge the cultural beliefs surrounding memory loss and cognition in aging. While recognizing the importance of family involvement, it is crucial to uphold the principle of individual autonomy in the decision-making process for research participation.
The I-CONECT study was a year-long protocol with multiple assessments and requirements, and many potential participants commented that it was too long or would take too much time. This was especially true since 50% of the Black/African American participants were no longer interested when assigned to the experimental group requiring 30-minute conversation sessions four days per week. The initial requirement of obtaining saliva samples proved unacceptable for some who feared how DNA information might be used. Finally, during our recruitment period, the COVID-19 pandemic mandated a research hiatus. The Midwest metropolitan area of the study was particularly hard hit by the pandemic resulting in significant delays in re-starting enrolled participants, and some participants were lost to follow-up.
Recruitment strategies that worked for White participants at the Pacific Coast site did not work at the Midwestern site. The enrolled Black participants came from multiple recruitment strategies with tiny yields compared to those from those efforts in the Pacific Coast site. Future studies should consider the significantly greater personnel time and cost of recruitment to yield results in the older old Black population.
Conclusions
Several conclusions can be drawn from our experience in the I-CONECT study. The definition of older old, mainly derived from studies of White participants, needs to consider the Black community wherein the life expectancy is reduced from that of Whites, limiting the comparisons between them using traditional age ranges. Recognizing the cultural and communication patterns of the Black older old population in defining social isolation is essential. While the study provided a rich opportunity to gather new information from an older old cohort, the many steps of the protocol proved onerous for the Black participants. While other studies have had significant success in church and health fairs/conferences recruitment activities,23–26 these methods were ineffective in finding the socially isolated Black older old adults.36 The sample demanded an underestimated proportion of study resources. Providing opportunities to engage family members in discussing the benefits and risks of a study for their older old relative is essential to the screening and consenting process. This may also decrease the time between contact and enrolment.37–40 It is hoped that lessons learned from this study will enhance future recruitment efforts for older old Black participants.
Clinical Implications
- Recognize there is diversity within the older old Black population and understanding cultural patterns as well as individuality is necessary when developing inclusion and exclusion criteria and study protocols.
- Multiple recruitment strategies, increased study personnel time, and an increased recruitment budget, is necessary for successful recruitment study participation. This includes in person visits with the potential subject and family member to explain the research and consenting process.
Data Sharing Statement
The I-CONECT study is a multi-site randomized controlled behavioral intervention trial (ClinicalTrial.gov: NCT02871921). The study protocol and its rationale are found at doi:10.3389/fight.2021.714813 and doi:10.1016/j.trci.2015.01.001.
Ethics Statement
The Institutional Review Board approved study procedures at the Oregon Health & Science University (OHSU) IRB STUDY00015937) using a single IRB process.
Acknowledgments
We are grateful to the I-CONECT study team for their contributions to the project. We also thank the study participants for their time, commitment, and interest.
Funding
The I-CONNECT study is supported by National Institute on Aging (NIA) Grant Nos. R01AG051628, R01AG056102, RO1AG056712,P30AG066518, P30AG024978,and P30AG053760.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alzheimer’s Association. 2018 Alzheimer’s disease facts and figures. Alzheimers Dement. 2018;14(3):367–429. doi:10.1016/j.jalz.2018.02.001
2. Ighodaro ET, Nelson PT, Kukull WA, et al. Challenges and considerations related to studying dementia in Blacks/African Americans. J Alzheimers Dis. 2017;60(1):1–10. doi:10.3233/JAD-170242
3. Bahls C Health policy brief: achieving equity in health. Health Aff. 2011;6:1–6. doi:10.1377/hpb20111006.957918/
4. Graff-Radford NR, Besser LM, Crook JE, Kukull WA, Dickson DW. Neuropathologic differences by race from the National Alzheimer’s Coordinating Center. Alzheimers Dement. 2016;12(6):669–677. doi:10.1016/j.jalz.2016.03.004
5. Shadlen MF, Siscovick D, Fitzpatrick AL, Dulberg C, Kuller LH, Jackson S. Education, cognitive test scores, and black‐white differences in dementia risk. J Am Geriatr Soc. 2006;54(6):898–905. doi:10.1111/j.1532-5415.2006.00747.x
6. Zuckerman IH, Ryder PT, Simoni-Wastila L, et al. Racial and ethnic disparities in the treatment of dementia among medicare beneficiaries. J Gerontol B Psychol Sci Soc Sci. 2008;63(5):S328–S333. doi:10.1093/geronb/63.5.S328
7. Franzen S, Smith JE, van den Berg E, et al. Diversity in Alzheimer’s disease drug trials: the importance of eligibility criteria. Alzheimers Dement. 2022;18(4):810–823. doi:10.1002/alz.12433
8. Gilmore-Bykovskyi A, Croff R, Glover CM, et al. Traversing the aging research and health equity divide: toward intersectional frameworks of research justice and participation. Gerontologist. 2022;62(5):711–720. doi:10.1093/geront/gnab107
9. Corbie-Smith G. The continuing legacy of the Tuskegee syphilis study: considerations for clinical investigation. Am J Med Sci. 1999;317(1):5–8. doi:10.1016/S0002-9629(15)40464-1
10. Rivers D, August EM, Sehovic I, Green BL, Quinn GP. A systematic review of the factors influencing African Americans’ participation in cancer clinical trials. Contemp Clin Trials. 2013;35(2):13–32. doi:10.1016/j.cct.2013.03.007
11. Grette KV, White AL, Awad EK, et al. Not immune to inequity: minority under-representation in immunotherapy trials for breast and gynecologic cancers. Int J Gynecol Cancer. 2021;31(11):1403–1407. doi:10.1136/ijgc-2021-002557
12. DeFilippis EM, Echols M, Adamson PB, et al. Improving enrollment of underrepresented racial and ethnic populations in heart failure trials: a call to action from the Heart Failure Collaboratory. JAMA Cardiol. 2022;7(5):540–548. doi:10.1001/jamacardio.2022.0161
13. Yu K, Wild K, Potempa K, et al. The Internet-based Conversational Engagement Clinical Trial (I-CONECT) in socially isolated adults 75+ years old: randomized controlled trial protocol and COVID-19 related study modifications. Front Digit Health. 2021;3:714813. doi:10.3389/fdgth.2021.714813
14. Dodge HH, Zhu J, Mattek NC, et al. Web-enabled conversational interactions as a method to improve cognitive functions: results of a 6-week randomized controlled trial. Alzheimer Dement. 2015;1(1):1–12. doi:10.1016/j.trci.2015.01.001
15. Lubben J, Blozik E, Gillmann G, et al. Performance of an abbreviated version of the Lubben social network scale among three European community-dwelling older adult populations. Gerontologist. 2006;46(4):503–513. doi:10.1093/geront/46.4.503
16. Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A short scale for measuring loneliness in large surveys: results from two population-based studies. Res Aging. 2004;26(6):655–672. doi:10.1177/0164027504268574
17. Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1982;17(1):37–49. doi:10.1016/0022-3956(82)90033-4
18. Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011;7(3):270–279. doi:10.1016/j.jalz.2011.03.008
19. Jack CR, Albert MS, Knopman DS, et al. Introduction to the recommendations from the national institute on aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer Dement. 2011;7(3):257–262. doi:10.1016/j.jalz.2011.03.004
20. McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer Dement. 2011;7(3):263–269. doi:10.1016/j.jalz.2011.03.005
21. Levkoff SE, Levy BR, Weitzman PF. The matching model of recruitment. J Ment Health Aging. 2000;6(1):29–38.
22. Levkoff S, Sanchez H. Lessons learned about minority recruitment and retention from the centers on minority aging and health promotion. Gerontologist. 2003;43(1):18–26. doi:10.1093/geront/43.1.18
23. Brown G, Marshall M, Bower P, Woodham A, Waheed W. Barriers to recruiting ethnic minorities to mental health research: a systematic review. Int J Methods Psychiatr Res. 2014;23(1):36–48. doi:10.1002/mpr.1434
24. Dreer LE, Weston J, Owsley C. Strategic planning for recruitment and retention of older African Americans in health promotion research programs. J Health Dispar Res Pract. 2014;7(2):14–33.
25. George S, Duran N, Norris K. A systematic review of barriers and facilitators to minority research participation among African Americans, Latinos, Asian Americans, and Pacific Islanders. Am J Public Health. 2014;104(2):e16–e31. doi:10.2105/AJPH.2013.301706
26. Graham LA, Ngwa J, Ntekim O, et al. Best strategies to recruit and enroll elderly blacks into clinical and biomedical research. Clin Interv Aging. 2018;13:43–50. doi:10.2147/CIA.S130112
27. Chadiha LA, Washington OG, Lichtenberg PA, Green CR, Daniels KL, Jackson JS. Building a registry of research volunteers among older urban African Americans: recruitment processes and outcomes from a community-based partnership. Gerontologist. 2011;51(3 Suppl 1):S106–S115. doi:10.1093/geront/gnr034
28. Kawas CH. The oldest old and the 90+ Study. Alzheimers Dement. 2008;4(1):S56–S59. doi:10.1016/j.jalz.2007.11.007
29. Paganini-Hill A, Kawas CH, Corrada MM. Activities and mortality in the elderly: the Leisure World Cohort Study. J Gerontol a Biol Sci Med Sci. 2011;66(5):559–567. doi:10.1093/gerona/glq237
30. Perry AB, Romer C, Barr A Why is life expectancy so low in Black neighborhoods? Brookings; 2021. Available from: https://www.brookings.edu/blog/the-avenue/2021/12/20/why-is-life-expectancy-so-low-in-black-neighborhoods/.
31. Taylor RJ, Chatters LM, Taylor HO. Race and objective social isolation: older African Americans, black Caribbeans, and non-Hispanic whites. J Gerontol B Psychol Sci Soc Sci. 2019;74(8):1429–1440. doi:10.1093/geronb/gby114
32. Finlay JM, Kobayashi LC. Social isolation and loneliness in later life: a parallel convergent mixed-methods case study of older adults and their residential contexts in the Minneapolis metropolitan area, USA. Soc Sci Med. 2018;208:25–33. doi:10.1016/j.socscimed.2018.05.010
33. Heu LC, Hansen N, van Zomeren M, et al. Loneliness across cultures with different levels of social embeddedness: a qualitative study. Pers Relatsh. 2021;28(2):379–405. doi:10.1111/pere.12367
34. Mody L, Miller DK, McGloin JM, et al. Recruitment and retention of older adults in aging research. J Am Geriatr Soc. 2008;56(12):2340–2348. doi:10.1111/j.1532-5415.2008.02015.x
35. Danner DD, Darnell KR, McGuire C. African American participation in Alzheimer’s disease research that includes brain donation. Am J Alzheimers Dis Other Demen. 2011;26(23):469–476. doi:10.1177/1533317511423020
36. Johnson JH, Appold SJ. US older adults: demographics, living arrangements, and barriers to aging in place. Kenan Institute; 2017:1–29. Available from: http://www.kenaninstitute.unc.edu/wp-content/uploads/2017/06/AgingInPlace_06092017.pdf.
37. Dyall L, Kepa M, Hayman K, et al. Engagement and recruitment of Māori and non-Māori people of advanced age to LiLACS NZ. Aust N Z J Public Health. 2013;37(2):124–131. doi:10.1111/1753-6405.12029
38. Pascucci MA, Chu N, Leasure AR. Health promotion for the oldest of old people. Nurs Older People. 2012;24(3):22–28. doi:10.7748/nop2012.04.24.3.22.c9017
39. Davies K, Collerton JC, Jagger C, et al. Engaging the oldest old in research: lessons from the Newcastle 85+ study. BMC Geriatr. 2010;10(1):1–9. doi:10.1186/1471-2318-10-64
40. Ewart CV, Fearon NA, Lund ME, et al. Subject recruitment, retention, and protocol feasibility in a prospective study of nutritional risk among urban, frail homebound elders. J Nutr Elder. 2001;21(1):1–21. doi:10.1300/J052v21n01_01
[ad_2]
Source link